


The Orbitozygomatic-Combined Supra- and Infratentorial Approach: Technical Note
Michael T. Lawton, MD
C. Phillip Daspit, MD†
Robert F. Spetzler, MD
Division of Neurological Surgery and Neuro-Otology† Barrow Neurological Institute, Mercy Healthcare Arizona, Phoenix, Arizona
Abstract
The orbitozygomatic-combined approach was applied in the case of a 60 year-old man with a large meningioma that spanned the anterior, middle, and posterior cranial fossae. The exposure provided by this approach enabled a radical resection of the tumor with preservation of all involved cranial nerves and vascular structures, and contributed to an excellent outcome. Compared to the standard combined approach, the additional anterior exposure of the orbitozygomatic-combined approach improved the safety and facility of tumor resection. This approach is ideal for lesions located at the center of the skull base that extend into all three cranial fossae and across the midline.
Key Words : combined supra- and infratentorial approach, meningioma, orbitozygomatic approach, skull base tumor, transcochlear approach
A critical component of many skull base approaches is the safe removal of the petrous bone.1-3,5-7,12-15,18,21,22,25,26,28 Petrosectomy opens a corridor of exposure to the center of the skull base. The transpetrosal approaches are familiar to most neurosurgeons and include the retrolabyrinthine,28 translabyrin-thine5,13,21 and transcochlear14,26 approaches. Still, exposure gained from these approaches can be limited at the region of interest medially or it can be inadequate for larger lesions. Therefore, transpetrosal approaches have been used in combination with other approaches to gain even more exposure. For example, the combined supra- and infratentorial approach joins the subtemporal and transpetrosal exposures to access the upper and middle clivus.7,12,25,2 The far-lateral combined supra- and infratentorial approach (combined-combined approach)3,4 adds to them the far-lateral exposure11,23,24,27 to access the entire clivus. We continue to experiment with combination approaches. One modification that has proven useful is the orbitozygomatic-combined supra- and infratentorial approach. Our experience with this modification is reported.
Case Report
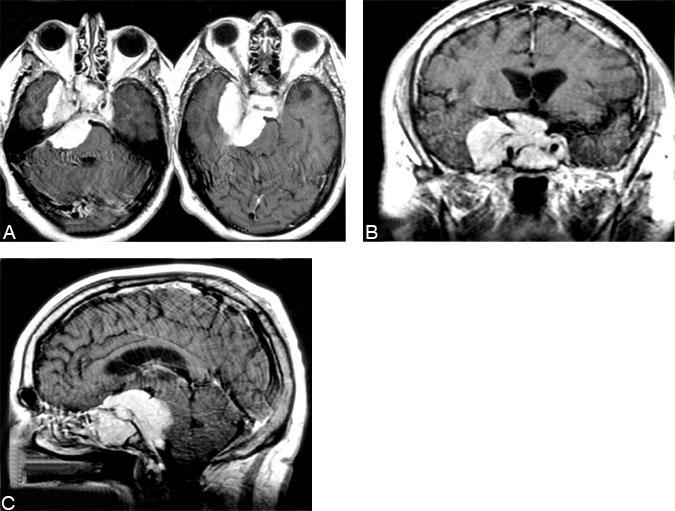
A 60-year-old male presented to the emergency room after a generalized tonic-clonic seizure. His only additional complaint was diplopia on right lateral gaze during the preceding month. His neurological examination was otherwise normal. In the medial right middle cranial fossa, magnetic resonance (MR) imaging demonstrated a 6 x 5 x 5-cm3 skull base tumor that enhanced homogeneously (Fig. 1). It extended anteriorly into the sella, sphenoid sinus, suprasellar cistern, and both right and left cavernous sinuses, and it encased both internal carotid arteries. Posteriorly, the tumor extended down to the pontomedullary junction, into the cerebellopontine angle and compressed the pons, right cerebellar peduncles, and right cerebral peduncle.
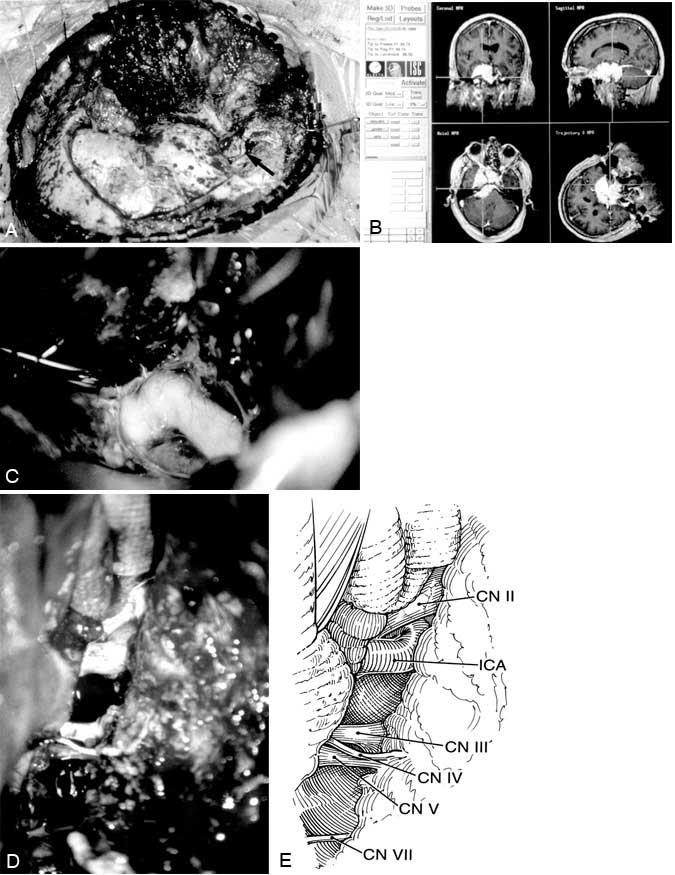
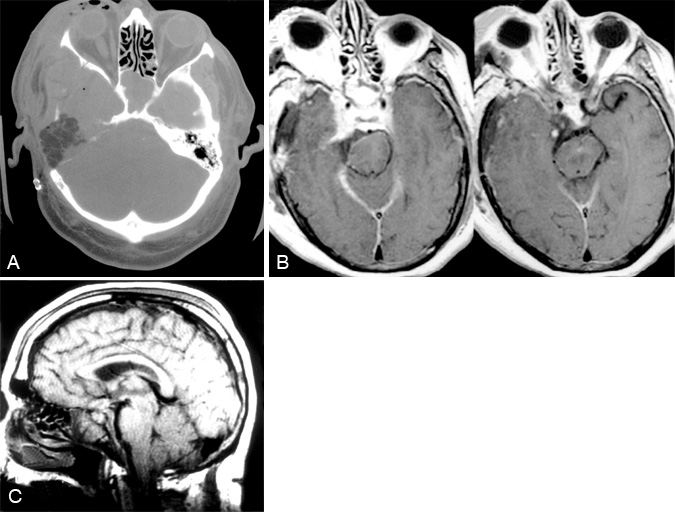
An orbitozygomatic-combined supra- and infratentorial approach with transcochlear petrosectomy was performed. Tumor encased the optic nerves, optic chiasm, pituitary stalk, internal carotid arteries, and the oculomotor, trochlear, trigeminal and abducent nerves and displaced the basilar artery and the facial and vestibulocochlear nerves. These neurovascular structures were dissected from the tumor, and all cranial nerves were left intact (Fig. 2). Resection of tumor in the cavernous sinus and sella was not attempted. Postoperative images demonstrated substantial tumor resection (Fig. 3). Meningioma was diagnosed by pathologic examination.
Postoperatively, the patient awoke with deficits of the oculomotor, facial, and vestibulocochlear nerves. He developed a communicating hydrocephalus that required a ventriculoperitoneal shunt. He made an excellent recovery. At a 1-year follow-up examination, function of the oculomotor nerve was normal and function of the facial nerve was almost normal.
Operative Technique
The patient is positioned supine with the head turned away from the lesion, bringing the midline parallel to the floor and inclined slightly downward. To expose the mastoid bone fully, the head is flexed to bring the chin to the contralateral shoulder. The skin incision begins at the mastoid tip, curves around the ear, and ends in the midline anteriorly at the hairline. The external auditory canal is transected and oversewn in two layers—a maneuver that allows the flap to be retracted anteriorly to the periosteum of the temporomandibular joint.
Petrosectomy is performed first. A basic mastoidectomy with complete removal of the bone covering the sigmoid sinus and dura of the posterior and middle fossae exposes the sinodural angle. The sigmoid sinus is unroofed inferiorly to the jugular bulb. The facial nerve is skeletonized along its mastoid segment and all three semicircular canals are removed. The internal auditory canal is skeletonized from the porus acousticus medially to Bill’s bar laterally. The wall of the posterior external auditory canal is taken down, and the ossicles and tympanic membrane are removed. The tympanic segment of the facial nerve is then exposed anteriorly to the geniculate ganglion. The greater superficial petrosal nerve is transected anteriorly at its origin from the geniculate ganglion, and the facial nerve is dissected from its bony canal and transposed posteriorly. The cochlea is drilled out completely. When the drilling is finished, the petrosectomy extends superiorly to the superior petrosal sinus and dura of the middle fossa floor, inferiorly to the jugular bulb and inferior petrosal sinus, anteriorly to the internal carotid artery, and medially to the carotid siphon and Meckel’s cave.
The orbitozygomatic craniotomy9, 10, 16, 17, 19, 20 is performed after the petrosectomy is completed. The fascia of the temporalis muscle is dissected in the subfascial plane, and the lateral orbital rim and zygoma are exposed deep to the nerves that supply the frontalis muscle. The entire zygoma is exposed from its root posteriorly to the malar eminence anteriorly, and the superior orbital rim is exposed medially to the notch of the supraorbital nerve. The temporalis muscle is elevated. The craniotomy begins behind the petrosectomy defect and sigmoid sinus and extends superiorly across the transverse sinus and anteriorly as a standard pterional flap. The orbitozygomatic osteotomies are made across the root of the zygoma, across the malar eminence from the inferior orbital fissure to the inferior zygoma, through the orbital roof lateral to the supraorbital nerve, and across the posterior orbit and pterion to the inferior orbital fissure. The orbitozygomatic bone is removed as a single piece.
The dura is incised in the shape of a “3,” with the anterior incision centered about the pterion and the posterior incision centered about the petrous bone. The incision simply joins a standard pterional dural flap with the dural incision of the combined approach. The latter begins over the temporal lobe, crosses the superior petrosal sinus below its entrance into the sigmoid sinus, and curves inferiorly in front of the sigmoid sinus to the jugular bulb. The superior petrosal sinus is coagulated and divided, and the tentorium is cut medially to the tentorial incisura and posteriorly to the trochlear nerve. This maneuver connects the supra- and infratentorial compartments and relaxes the neural structures. The petroclival region, brain stem, cranial nerves, and blood vessels of the posterior circulation are exposed (Fig. 2) and the pathology can be accessed.
Meticulous dural closure and an abdominal fat graft in the petrosectomy defect are important factors in preventing a postoperative cerebrospinal fluid leak. The resected orbitozygomatic bone and the bone flap are fixated with plates and screws.
Discussion
We categorize the transpetrosal approaches into three variations: retrolabyrinthine, translabyrinthine, and transcochlear.26, 28 The retrolabyrinthine approach removes temporal bone between the semicircular canals anteriorly and the dura of the posterior fossa on the posterior aspect of the temporal bone. The translabyrinthine approach removes the semicircular canals, which increases the exposure anteriorly to the internal auditory canal but causes hearing loss.5, 13 The transcochlear approach, which requires transposition of the facial nerve to gain access to the cochlea for its removal, enables almost complete removal of the petrous bone.14 The three types of temporal bone dissections represent a graduated increase in the amount of petrous bone resected with a corresponding increase in anterior exposure. The price of this increased exposure is progressively greater sacrifice of function of the facial and vestibulocochlear nerves.
Combination approaches build on the transpetrosal approaches to provide even greater exposure for complex lesions. The combined supra- and infratentorial approach7, 25, 26 adds a craniotomy that begins above the petrosectomy defect over middle fossa dura, courses across the transverse sinus, and ends behind the petrosectomy defect over posterior fossa dura. After the dura has been opened and the tentorium divided medially to the hiatus, the supra- and infratentorial compartments are connected and extensive exposure of the petroclival region and associated neurovascular structures is obtained with minimal brain retraction. When petroclival lesions span the entire length of the posterior fossa to the foramen magnum, a far-lateral combined supra- and infratentorial (combined-combined) approach may be indicated.3, 4 The far-lateral approach is simply a lateral extension of a unilateral suboccipital approach that removes additional lateral occipital bone, the inferior foramen magnum, the posterior half of the condyle, and the arch of the first cervical vertebra.11, 23, 27 The combined-combined approach joins the transpetrosal, subtemporal, and far-lateral approaches and is the most extensive of the combination approaches. It exposes the entire petroclival region; anterolateral brain stem; third through twelfth cranial nerves; and the basilar, vertebral, and anterior spinal arteries.8
None of these combinations adequately exposes the parasellar region for lesions that span all three cranial fossae. Combination approaches without an orbitozygomatic osteotomy are limited to subtemporal exposure of the middle cranial fossa, and they provide no exposure of the anterior cranial fossa. The orbitozygomatic-combined supra- and infratentorial approach arose from continued experimentation with new combination approaches to gain additional exposure of the middle and anterior cranial fossae. In recent years we have used the orbitozygomatic approach extensively to gain upward exposure of basilar tip aneurysms that extend above the posterior clinoid processes and to access cavernous malformations that surface on the anterior midbrain. The orbitozygomatic-combined approach widely exposes all three cranial fossae. A lesion at the center of the skull base that encases important arteries and cranial nerves can be accessed from various angles to optimize the dissection of these structures and the chances of their preservation.
The orbitozygomatic-combined approach is indicated for large tumors of the middle fossa that extend forward to the anterior cranial fossa floor, down to the lower third of the clivus, and across the midline to involve the contralateral optic nerve and carotid artery. The petrosectomy is needed to access the inferior part, and the orbitozygomatic osteotomy is needed to access the anterior part of the lesion. The approach is well-suited for tumors that extend high in the middle fossa, because removing the orbital roof and zygomatic arch gives the surgeon an upward viewing angle over the top of the lesion from either the front or the side. Although we have not had occasion to use this approach more than once, it is ideal for these rare and complex skull base lesions. The simple addition of a more anterior craniotomy and the orbitozygomatic osteotomy greatly facilitates tumor removal.
References
- Al-Mefty O, Fox JL, Rifai A, et al: A combined infratemporal and posterior fossa approach for the removal of giant glomus tumors and chondrosarcomas. Surg Neurol 28:423-431, 1987
- Al-Mefty O, Fox JL, Smith RR: Petrosal approach for petroclival meningiomas. Neurosurgery 22:510-517, 1988
- Baldwin HZ, Miller CG, van Loveren HR, et al: The far lateral/combined supra- and infratentorial approach. A human cadaveric prosection model for routes of access to the petroclival region and ventral brain stem. J Neurosurg 81:60-68, 1994
- Baldwin HZ, Spetzler RF, Wascher TM, et al: The far lateral-combined supra- and infratentorial approach: Clinical experience. Acta Neurochir (Wien) 134:155-158, 1995
- Brackmann DE, Green JD: Translabyrinthine approach for acoustic tumor removal. Otolaryngol Clin North Am 25:311-329, 1992
- Brackmann DE, House JR, III, Hitselberger WE: Technical modifications to the middle fossa craniotomy approach in removal of acoustic neuromas. Am J Otol 15:614-619, 1994
- Daspit CP, Spetzler RF, Pappas CTE: Combined approach for lesions involving the cerebellopontine angle and skull base: Experience with 20 cases—preliminary report. Otolaryngol Head Neck Surg 105:788-796, 1991
- de Oliveira E, Rhoton AL, Jr., Peace D: Microsurgical anatomy of the region of the foramen magnum. Surg Neurol 24:293-352, 1985
- Hakuba A, Liu S, Nishimura S: The orbitozygomatic infratemporal approach: A new surgical technique. Surg Neurol 26:271-276, 1986
- Hakuba A, Tanaka K, Suzuki T, et al: A combined orbitozygomatic infratemporal epidural and subdural approach for lesions involving the entire cavernous sinus. J Neurosurg 71:699-704, 1989
- Heros RC: Lateral suboccipital approach for vertebral and vertebrobasilar artery lesions. J Neurosurg 64:559-562, 1986
- Hitselberger WE, House WF: A combined approach to the cerebellopontine angle. A suboccipital-petrosal approach. Arch Otolaryngol 84:267-285, 1966
- House WF: Translabyrinthine approach, in House WF, Luetje CM (eds): Acoustic Tumors. Vol. 2: Management. Baltimore: University Park, 1979, pp 43-87
- House WF, Hitselberger WE: The transcochlear approach to the skull base. Arch Otolaryngol 102:334-342, 1976
- House WF, Shelton C: Middle fossa approach for acoustic tumor removal. Otolaryngol Clin North Am 25:347-359, 1992
- Ikeda K, Yamashita J, Hashimoto M, et al: Orbitozygomatic temporopolar approach for a high basilar tip aneurysm associated with a short intracranial internal carotid artery: A new surgical approach. Neurosurgery 28:105-110, 1991
- Jane JA, Park TS, Pobereskin LH, et al: The supraorbital approach: Technical note. Neurosurgery 11:537-542, 1982
- Kawase T, Toya S, Shiobara R, et al: Transpetrosal approach for aneurysms of the lower basilar artery. J Neurosurg 63:857-861, 1985
- Lee JP, Tsai MS, Chen YR: Orbitozygomatic infratemporal approach to lateral skull base tumors. Acta Neurol Scand 87:403-409, 1993
- McDermott MW, Durity FA, Rootman J, et al: Combined frontotemporal-orbitozygomatic approach for tumors of the sphenoid wing and orbit. Neurosurgery 26:107-116, 1990
- Morrison AW, King TT: Experiences with a translabyrinthine-transtentorial approach to the cerebello-pontine angle. J Neurosurg 38:382-390, 1973
- Sekhar LN, Kalia KK, Yonas H, et al: Cranial base approaches to intracranial aneurysms in the subarachnoid space.Neurosurgery 35:472-483, 1994
- Sen CN, Sekhar LN: An extreme lateral approach to intradural lesions of the cervical spine and foramen magnum. Neurosurgery 27:197-204, 1990
- Sen CN, Sekhar LN: Surgical management of anteriorly placed lesions at the craniocervical junction—an alternative approach.Acta Neurochir (Wien) 108:70-77, 1991
- Spetzler RF, Daspit CP, Pappas CTE: Combined approach for lesions involving the cerebellopontine angle and skull base: Experience with 30 cases. Skull Base Surg 1:226-234, 1991
- Spetzler RF, Daspit CP, Pappas CTE: The combined supra- and infratentorial approach for lesions of the petrous and clival regions: Experience with 46 cases. J Neurosurg 76:588-599, 1992
- Spetzler RF, Grahm T: The far-lateral approach to the inferior clivus and the upper cervical region: Technical note. BNI Quarterly 6:35-38, 1990
- Spetzler RF, Hamilton MG, Daspit CP: Petroclival lesions. Clin Neurosurg 41:62-82, 1994