


Dementing Lewy Body Disease: Review of the Literature
Authors
D. Larry Sparks, PhD*
Ronald J. Lukas, PhD†
Denise A. Drumm, PhD‡
*L. J. Roberts Alzheimer’s Center, Sun Health Research Institute, Sun City, Arizona
†Division of Neurobiology, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
‡Civin Neuropathology Laboratory, Sun Health Research Institute, and Barrow Neurological Institute, Phoenix, Arizona
Abstract
Lewy body disease, a distinct clinical and neuropathological entity, is the second most common dementing disorder. This article reviews recent advances in the characterization of Lewy body disease. Clinical, pathological, genetic, neurochemical, and pharmacological features of Lewy body and other dementing diseases are compared and contrasted.
Key Words : Alzheimer’s disease, choline acetyltransferase, dementia, dopamine, hallucinations, Lewy body, neurodegeneration, Parkinson’s disease, serotonin
Postmortem examinations indicate that Lewy bodies are found in the brain tissue of approximately 20% of all demented patients.67, 77As a distinct entity, Lewy body disease is the second most common classification of dementing disorders.20,48,55 Nevertheless, the neuropathology of Lewy bodies is invariably considered in relation to the neuropathology of Alzheimer’s disease, the most common cause of dementing illness. Individuals with neuropathology related to both Alzheimer’s disease and Lewy body disease are considered to have the Lewy body variant of Alzheimer’s disease, also known as senile dementia of the Lewy body type. However, individuals with Lewy body dementia associated with little or no Alzheimer’s disease-like neuropathology, a condition known as pure diffuse Lewy body disease, comprise 20% of all cortical Lewy body cases.53,54
Lewy bodies have been observed in patients with Down’s syndrome, an eventually dementing condition neuropathologically similar to Alzheimer’s disease.9,80 Lewy bodies are also reported as incidental neuropathological findings in a variety of other disorders: Meige’s (Milroy’s) disease,56,63 progressive supranuclear palsy (Steele-Richardson-Olszewski disease),23,70 Hallervorden-Spatz disease,2,34,93 pure autonomic failure,95 Joseph disease,34 olivopontocerebellar atrophy,44 REM (rapid eye movement) sleep behavior disorder,94 infantile and juvenile neuroaxonal dystrophy,40 motor neuron disease,65 subacute sclerosing panencephalitis,32 and ataxia-telangiectasia.35 They also are found in very old but cognitively normal individuals,6,78 where they may represent a preclinical stage of senile dementia of the Lewy body type.78
Among the foregoing disorders, there is no direct evidence that the reported inclusions are true Lewy bodies (identical to the Lewy bodies associated with Parkinson’s disease or diffuse Lewy body disease) or Lewy body-like structures. For example, Lewy body-like neuronal inclusions reported in both sporadic and familial amyotrophic lateral sclerosis49,58 are likely different than those associated with Parkinson’s disease and diffuse Lewy body disease. The Lewy body neuronal inclusion is rarely the sole neuropathological lesion observed in an individual’s brain (excluding Parkinson’s disease),46 but a number of clinical, pathological, chemical, and pharmacologic sequelae distinguish the dementia of Lewy body disease from other dementing disorders.
Recently, consensus guidelines were established for the clinicopathologic diagnosis of dementing Lewy body disease.68 To review the literature, however, the previous nomenclature was used to classify demented patients with Lewy bodies in the brain. For these purposes, we define four basic neuropathological categories of Lewy body disease. The first category is Parkinson’s disease with or without dementia. In this category cortical Lewy bodies can occur in patients with Parkinson’s disease in the absence of dementia.17They can also be absent in patients with Parkinson’s disease with dementia. Brain stem nigral Lewy bodies, however, occur in all patients with Parkinson’s disease whether or not dementia is present.
{kind=link}

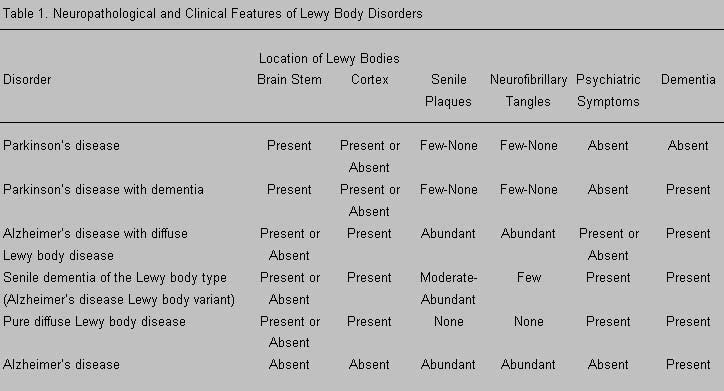
The second category is neuropathologically confirmed Alzheimer’s disease with Parkinson’s disease (brain stem nigral Lewy bodies only) or with diffuse cortical or cortical plus brain stem Lewy bodies. In the third category, senile dementia of the Lewy body type (or the Lewy body variant of Alzheimer’s disease), cortical and brain stem Lewy bodies and numerous senile plaques are present, but there are very few cortical neurofibrillary tangles (NFTs). In the fourth category, diffuse Lewy body disease, Lewy bodies are found cortically and subcortically and, for the most part, in the brain stem. Essentially, there are no neuropathological features of Alzheimer’s disease in pure diffuse Lewy body disease (Table 1). This article compares and contrasts all of these diseases with Alzheimer’s disease without Lewy bodies.
According to the newly established consensus guidelines, any dementing disorders featuring Lewy bodies are to be lumped together and called ‘dementia with Lewy bodies,’ regardless of any other simultaneous neuropathological diagnosis.68 This category includes all the subgroups discussed: Parkinson’s disease with dementia, Alzheimer’s disease with Parkinson’s disease, Alzheimer’s disease with diffuse Lewy body disease, the Lewy body variant of Alzheimer’s disease, senile dementia of the Lewy body type, and pure diffuse Lewy body disease. The new consensus guidelines provide a numerical staging system from which three subtypes of dementia with Lewy bodies are derived and grouped according to the distribution of Lewy bodies in the brain.68 These groupings include brain stem predominant, limbic predominant, and cortical predominant, where five or more Lewy bodies in any cortical region would constitute cortical dementia with Lewy bodies.68
Clinical Features
Patients with Lewy body dementia exhibit a more rapid disease course compared to those with Alzheimer’s disease.4,5 The age of onset is younger in patients with pure diffuse Lewy body disease compared to those diagnosed with the Lewy body variant of Alzheimer’s disease.12 As a result of the rapid progression of Lewy body dementia, its clinical manifestations, such as the onset of urinary incontinence, may emerge earlier in patients with pure diffuse Lewy body disease than in those with the Lewy body variant of Alzheimer’s disease.18
Clinically, psychiatric disturbances may be present before dementia in patients with diffuse Lewy body disease and those with senile dementia of the Lewy body type or the Lewy body variant of Alzheimer’s disease. Most investigators have reported that the cognitive changes in patients with dementing Lewy body disease fluctuate.11,15,20,48,67,69 Other studies have suggested that depression appears early in the course of dementing diffuse Lewy body disease.33,77
Psychiatric alterations and dementia are also reported to precede symptoms of Parkinson’s disease in patients with Lewy body disease who exhibit a movement disorder.10 Patients with pure diffuse Lewy body disease can become symptomatic with parkinsonian symptoms followed by hallucinations and then dementia, or they can become symptomatic with dementia and hallucinations and then develop parkinsonian symptoms.42 This progression may be related to the neuropathological presence of Lewy bodies first in the brain stem and then in the neocortex rather than first in the neocortex and then in the brain stem.42
When patients with Alzheimer’s disease were compared to those with the Lewy body variant of Alzheimer’s disease matched for the severity of their dementia, greater deficits in attention, fluency, and visuospatial processing were apparent in the latter.37 Likewise, the ability to copy figures (i.e., clocks, cubes, and crosses) was dramatically decreased in mildly demented patients with the Lewy body variant of Alzheimer’s disease compared to equally demented patients with Alzheimer’s disease alone.27
The prevalence of psychiatric disturbances may be greater in patients with diffuse Lewy body disease than in those with Alzheimer’s disease98 although at least one study has reported no difference in this dimension between the two groups.25 A recent study compared patients with diffuse Lewy body disease, Alzheimer’s disease, and Parkinson’s disease. The prevalence of depression was higher in patients with diffuse Lewy body disease than in those with Alzheimer’s disease, as was the prevalence of hallucinations. Delusions were equally common in these two groups, but their incidence was much higher than in patients with Parkinson’s disease alone.51 Even among nondemented elderly individuals, the presence of a psychiatric disturbance may be related to the incidence of cerebral Lewy bodies.78
As found in patients with Alzheimer’s disease, positron emission tomography (PET) with fluoro-deoxyglucose in individuals with the Lewy body variant of Alzheimer’s disease or with diffuse Lewy body disease has shown reduced metabolism in the association cortex while the primary somatosensory and motor cortex and subcortical regions were spared.1 In contrast to patients with Alzheimer’s disease, decrements in glucose metabolism were identified in the occipital and primary visual cortex of patients with diffuse Lewy body disease.1 When single-photon emission tomography was used to evaluate cerebral perfusion, similar findings were reported in the occipital and primary visual cortex of patients with diffuse Lewy body disease compared to those with Alzheimer’s disease.20Furthermore, studies using functional magnetic resonance (MR) imaging have suggested that reduced activation in the primary visual cortex may be related to the hallucinations that occur in patients with Lewy body dementia.43
The dementia of Lewy body disease may correlate with the number of Lewy bodies in a number of cortical areas in patients with the Lewy body variant of Alzheimer’s disease.85 Despite comparable densities of Lewy bodies, dementia is less severe in patients with pure diffuse Lewy body disease compared to those with the Lewy body variant of Alzheimer’s disease.84
{kind=link}

Pathological Features
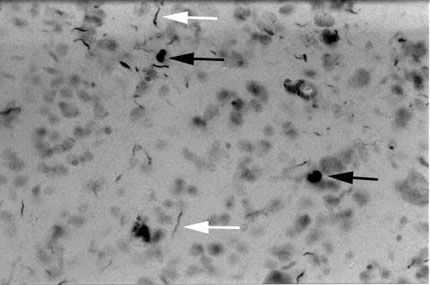
Lewy bodies are eosinophilic cytoplasmic neuronal inclusions. Microscopically, their appearance varies, depending on where they occur in the brain. Thus far, Lewy bodies have been found in the hypothalamus,10 cerebellum,100 dorsal motor nucleus of the vagus,79 cortex,79,81 hippocampus,81 amygdala,79,81 basal forebrain (nucleus basalis of Meynert), and brain stem where Lewy bodies not confined to the cell body can be axonal or dendritic.79 In the brain stem, Lewy bodies most often appear to have a dense core surrounded by a pale halo. In the cortex, Lewy bodies are often irregular spheroids and rarely have a halo (Fig. 1). The neuronal inclusions called pale bodies16,36 may be a precursor or early form of Lewy bodies.14,16 Neuronal accumulations of neurotransmitter monoamines may also be precursors to Lewy bodies and therefore possibly an earlier form of pale bodies.86 Ghost Lewy bodies (Lewy bodies free in the extracellular spaces) are rare92 but have been reported.14,24,47
Lewy bodies contain ubiquitin29,79 and neurofilament proteins, which recently have been shown to be primarily of an intermediate length.30 Although Lewy bodies are not immunoreactive with tau79 or Alz-50 antibody,15,79 they are immunoreactive with other proteins such as a-synuclein,91 complement,99 and microtubule-associated protein 5 (MAP-5).26 In addition, Lewy bodies in the cell body of a neuron are immunoreactive with microtubule-associated protein-2 (MAP-2) but rarely with synaptic vesicle protein (SVP-38). Conversely, axonal Lewy bodies show significantly more SVP-38 immunoreactivity than MAP-2 immunoreactivity.97 This finding may suggest that the number of dense core vesicles in a Lewy body-containing neuron is more likely related to the neuron’s stage of degeneration than to the stage of Lewy body disease.97 The later the stage of neurodegeneration in Lewy body disease, the fewer the number of dense core vesicles there are in a Lewy body-containing neuron.97
Lewy bodies also house synaptic proteins, and synaptic protein profiles are lost in patients with the Lewy body variant of Alzheimer’s disease and diffuse Lewy body disease. This finding has prompted the suggestion that such synaptic proteins are involved in the formation of Lewy bodies.96 In contrast, there is no correlation between the severity of dementia in Lewy body disease and a marker for synaptic contacts, synaptophysin immunoreactivity.84
One group has reported that in the cortex the greatest density of Lewy bodies is in the parahippocampal gyrus followed by the middle temporal gyrus, cingulate cortex, insular cortex, superior temporal gyrus, superior frontal cortex, and the parietal and occipital cortex.81 This same group has suggested that the number of Lewy bodies in the brain stem (substantia nigra) is somewhat more dense than in the parahippocampal gyrus, and the numbers of Lewy bodies in CA1 of the hippocampus and the nucleus basalis of Meynert are equivalent to the numbers found in the superior temporal gyrus.81 These findings are open to debate. We agree that the greatest density of Lewy bodies in the brain is found in the amygdala (Sparks DL et al., unpublished data, 1998).81 Our studies, however, suggest that the density of Lewy bodies in the temporal pole is equivalent to that in the amygdala (Sparks DL et al., unpublished data, 1998).
Ubiquitinated neuropil threads or neurites also occur in dementing Lewy body disease (i.e., diffuse Lewy body disease, the Lewy body variant of Alzheimer’s disease or senile dementia of the Lewy body type, and Alzheimer’s disease with diffuse Lewy body disease). The presence of ubiquitin immunoreactive threads in CA2 and CA3 of the hippocampus may be an indicator of Lewy bodies in the cortex.19 Ubiquitin-immunoreactive granules and neurites can be visualized because the neurons of origin may degenerate more rapidly in diffuse Lewy body disease than in Alzheimer’s disease or the Lewy body variant of Alzheimer’s disease.45 The presence of ubiquitin-immunoreactive elements in the transentorhinal and entorhinal cortex and the amygdala may reflect degeneration of terminals or distal axons of neurons in the perforant pathway.45
The presence of Lewy bodies in diffuse Lewy body disease seems to correlate with the presence of neuritic senile plaques but not with NFTs,81 while the concentration of the amyloid precursor protein, which is an antecedent to senile plaques, is increased in neurons that contain Lewy bodies.32 At the same time, increased GAP-43 immunoreactivity is associated with more senile plaques in Lewy body disease than in Alzheimer’s disease.64 Because GAP-43 is a marker of neuritic outgrowth and neuronal sprouting, this observation may indicate an early response to neuronal damage and may differentiate Alzheimer’s disease from Lewy body disease.64
Neuronal loss is also associated with dementia in individuals with cortical Lewy bodies. When patients with Alzheimer’s disease are compared with those with the Lewy body variant of Alzheimer’s disease matched for severity of dementia, there is a greater loss of neurons in the substantia nigra, locus ceruleus, and nucleus basalis of Meynert and fewer NFTs in the latter.37 Isolated regions of changes in spongiform tissue occur in demented subjects with cortical Lewy bodies, but there is no evidence of prion, protein, or disease transmissibility as in Creutzfeldt-Jacob disease.79
Genetic Features
Familial Parkinson’s disease was first noted by Mjones and subsequently discounted. Reevaluation, however, supported an autosomal dominant transmission with approximately 60% penetrance.21 An autosomal dominant family exhibiting parkinsonism with depression has now been reported,8 as well as a family with autosomal dominant parkinsonism with cortical Lewy bodies and neurites in CA2 and CA3 of the hippocampus.48 Linkage studies for monoamine oxidase-A and debrisoquine hydroxylase are underway. Tyrosine hydroxylase has been excluded in familial juvenile Parkinson’s disease.21 Further studies have indicated that debrisoquine hydroxylase mutant allele is overrepresented in the Lewy body variant of Alzheimer’s disease.83 The allele is also found in Parkinson’s disease.3,52,57,88 The effect of debrisoquine hydroxylase mutations in pure diffuse Lewy body disease remains to be identified.
The frequency of the apolipoprotein E epsilon 4 allele (ApoE-e4) is increased in Alzheimer’s disease.71,82,87,90 Because of its possible overlap with Alzheimer’s disease, the genetics of apolipoprotein E has been studied extensively in Lewy body disease. In comparative studies, ApoE-e4 is overrepresented in Alzheimer’s disease and the Lewy body variant of Alzheimer’s disease28,50 but not in pure diffuse Lewy body disease, where its frequency equals the frequency of control alleles.28 Furthermore, the frequency of the ApoE-e4 allele in Parkinson’s disease with Alzheimer’s disease is equal to its frequency in Parkinson’s disease alone, which in turn is equal to its frequency in control alleles.22 Interestingly, the ApoE-e2/3 genotype may be overrepresented in diffuse Lewy body disease (frequency of 0.25)28 as it is in vascular dementia (frequency of 0.211).7 Parenthetically, this overrepresentation could be related to the fluctuation of symptoms that occur in both diffuse Lewy body disease and vascular dementia.
Another group has confirmed an increase in the frequency of the e2 allele (0.14) and a slight increase in the frequency of e4 (0.22) in a group of patients with diffuse Lewy body disease who did not meet the criteria for Alzheimer’s disease with diffuse Lewy body disease compared to control patients.62 In patients with the diffuse Lewy body disease, neuritic degeneration in CA2 and CA3 of the hippocampus and increased amyloid plaques may be related to the ApoE genotype.62
In yet another study, the number of NFTs in patients with the Lewy body variant of Alzheimer’s disease increased with the occurrence of the ApoE-e4 allele but not in patients with Alzheimer’s disease alone. A threshold or ceiling effect may be involved.38 This finding is similar to the effect of the increased frequency of the ApoE-e4 allele on the density of NFTs in nondemented individuals with hypertension—they have a prematurely enhanced prevalence of NFTs. In patients with Alzheimer’s disease, the ApoE genotype does not appear to affect NFTs.89
The frequency of the ApoE-e4 allele appears to be similar in patients with Alzheimer’s disease (0.328) and those with senile dementia of the Lewy body type (0.365; the Lewy body variant of Alzheimer’s disease) and in patients with Parkinson’s disease with or without dementia (0.098) compared to controls (0.147).39 A different group of investigators has confirmed an increase in the frequency of the ApoE-e4 allele in patients with Alzheimer’s disease and the Lewy body variant of Alzheimer’s disease, but they suggested that the frequency of the allele was increased in patients with Parkinson’s disease with dementia compared to those with only Parkinson’s disease.41
Overall, the data indicate there is no relationship between pure Parkinson’s disease or diffuse Lewy body disease and the frequency of ApoE-e4. There is, however, a relationship between the ApoE-e4 genotype and Alzheimer’s disease, regardless of whether Lewy bodies are present.
Neurochemical Features
Dopaminergic Markers
The reduction of markers for dopaminergic neurotransmission in the basal ganglia of patients with Parkinson’s disease is well-known. When patients with the Lewy body variant of Alzheimer’s disease are compared to those with Alzheimer’s disease alone, the reductions of dopamine and its metabolite homovanillic acid in the basal ganglia (caudate nucleus and putamen) are more severe in the former.59 In contrast, decreases in levels of dopamine and homovanillic acid in cortical areas are not significant, and there is no difference in their levels between patients with the Lewy body variant of Alzheimer’s disease and those with Alzheimer’s disease alone.59 Levels of dopamine and homovanillic acid in the caudate nucleus of patients with senile dementia of the Lewy body type are reduced midway between the levels found in patients with Parkinson’s disease and Alzheimer’s disease. Furthermore, the level of each is significantly lower than is found in control patients.75 In the temporal cortex, the levels of homovanillic acid are lower in nonhallucinating patients with senile dementia of the Lewy body type than in hallucinating patients with the same disorder or the control patients.74 Based on PET, the transport of dopamine is lower in patients with diffuse Lewy body disease than in those with Alzheimer’s disease.20
Cholinergic Markers
The neurotransmitter acetylcholine is synthesized by the enzyme choline acetyltransferase (ChAT) and interacts at both nicotinic and muscarinic receptors in the brain. A single-point analysis of ChAT activity (one concentration of a substrate for enzymatic modification) in the caudate nucleus and putamen of patients with Alzheimer’s disease and those with the Lewy body variant of Alzheimer’s disease has been performed. Enzymatic levels were equally reduced in the caudate of both groups compared to controls, but there was no difference in the putamen among the three groups.59
Investigations of nicotinic receptor binding show no changes in the putamen and caudate nucleus of patients with senile dementia of the Lewy body type or Parkinson’s disease compared to control patients.76 In contrast, the density of nicotinic receptors is reduced in the brain stem of patients with senile dementia of the Lewy body type or Parkinson’s disease but not in those of patients with Alzheimer’s disease.76 Nicotinic binding is reduced in the hippocampus of patients with Lewy body disease or Alzheimer’s disease but not in those with Parkinson’s disease; binding is reduced in the parahippocampal gyrus in patients with Alzheimer’s disease but not in patients with Lewy body disease.76
In the temporal lobe, nicotinic receptors are reduced in all cortical layers of patients with Alzheimer’s disease but only in the deep layers of patients with Lewy body disease. This finding may reflect the prevalence of Lewy bodies in the deep cortical layers in Lewy body disease.76 The number of nicotinic receptors is reduced in the temporal and parietal cortex of patients with senile dementia of the Lewy body type or Alzheimer’s disease compared to controls.
Muscarinic receptor binding is increased in the temporal, parietal, and occipital cortex in patients with senile dementia of the Lewy body type but not in those with Alzheimer’s disease.73 Furthermore, the number of type-L muscarinic receptors increases proportionately as ChAT decreases in the cortex of patients with senile dementia of the Lewy body type.75
Single-point analysis of ChAT in the lateral parietal cortex (Brodmann areas 39 and 40) of patients with senile dementia of the Lewy body type demonstrated a reduction in its activity midway between the decrements found in patients with Parkinson’s disease and those with Alzheimer’s disease. For all three disorders, ChAT activity was lower than in controls.75
Another single-point analysis has suggested that ChAT activity in the frontal cortex is more severely decreased in patients with the Lewy body variant of Alzheimer’s disease than in those with Alzheimer’s disease alone. ChAT activity considerably overlaps in the temporal cortex of these two groups and is quite variable in the parietal and occipital cortex.60 The level of ChAT activity in the neocortex was decreased more in the midfrontal and lateral parietal cortex of patients with the Lewy body variant of Alzheimer’s disease compared to those with Alzheimer’s disease matched for severity of dementia. In the superior temporal cortex, however, there was no difference in the level of ChAT activity in patients with the Lewy body variant of Alzheimer’s disease and those with Alzheimer’s disease.37
Although ChAT activity is reduced in the frontal cortex (area 8) of patients with both the Lewy body variant of Alzheimer’s disease and Alzheimer’s disease alone, the reduction is greatest in the former. Compared to controls, ChAT activity is reduced in both the temporal (area 21) and the parietal cortex (areas 39 and 40). The differences, however, are not significant.59
ChAT activity is decreased more in the frontal, temporal, and occipital cortex of patients with Alzheimer’s disease with diffuse Lewy body disease compared to those with Alzheimer’s disease alone.72 The cholinergic levels do not correlate with the density of Lewy bodies.72 Furthermore, decreases in ChAT activity in the frontal cortex were greater in patients with Alzheimer’s disease alone than in those with Alzheimer’s disease with diffuse Lewy body disease.72 The levels of ChAT activity were lower in the temporal and parietal cortex of patients with senile dementia of the Lewy body type than in those with Alzheimer’s disease, but the difference was only significant if the patients with Lewy body disease experienced hallucinations.72
Because some patients with Lewy body disease experience hallucinations, a number of studies have attempted to determine the chemical differences between patients with and without psychiatric symptoms. In the temporal cortex (areas 21 and 22), hallucinating patients with senile dementia of the Lewy body type show a greater decrease in ChAT activity than nonhallucinating patients. Activity in both groups, however, was significantly lower than in control patients.74 The density of nicotinic receptors is most reduced in hallucinating patients with senile dementia of the Lewy body type, while the number of muscarinic receptors increased equally in both hallucinating and nonhallucinating subjects.74
In another single-point study, the level of ChAT activity in the frontal, temporal, parietal, and entorhinal cortex or hippocampus was not significantly different in patients with senile dementia of the Lewy body type or those with Alzheimer’s disease. In the occipital cortex, the level of ChAT activity in these two groups was no different than in controls.73 Compared to nonhallucinating subjects with senile dementia of the Lewy body type, ChAT activity was lower in the parietal, temporal and frontal cortex but not in the occipital cortex of hallucinating subjects with the same disorder.73 In yet another study, the only difference between hallucinating and nonhallucinating patients with senile dementia of the Lewy body type was reduced levels of ChAT in the parietal cortex (areas 39 and 40) of the hallucinating subjects.75
Despite all these studies on cholinergic indices in Lewy body disease, there is no consensus about the effect of such cholinergic markers when such patients are compared to those with Alzheimer’s disease. Most, but not all studies, suggest that the decrements in ChAT activity in the frontal cortex are more severe in Lewy body disease than in Alzheimer’s disease, and that ChAT activity may be diminished in the temporal cortex if a patient with Lewy body disease experiences hallucinations.
The main caveat associated with the foregoing studies is that none of the investigators performed kinetic analyses of ChAT enzymatic activity. Yet, small differences in the concentrations of substrate used to analyze enzymatic activity in a single-point analysis could have dramatic effects on the differences observed among groups. Comparing single-point data from patients with diffuse Lewy body disease to those with Alzheimer’s disease with diffuse Lewy body disease or those with the Lewy body variant of Alzheimer’s disease, we found enhanced but nonsignificant decrements of ChAT activity in the amygdala and temporal and frontal cortex (Sparks DL, et al., unpublished data, 1998). Kinetic analysis of enzyme activity, however, has shown no differences among any groups in any area of the brain investigated (Sparks DL, et al., unpublished data, 1998). Likewise, the outcome of kinetic analysis in patients with Lewy body disease with and without hallucinations has revealed no differences in the level of ChAT activity between the two groups (Sparks DL, et al., unpublished data, 1998).
Serotonergic Markers
Few studies of serotonergic markers in patients with dementia of Lewy body disease have been performed. Levels of the neurotransmitter serotonin (5HT) are decreased in the caudate nucleus and putamen of patients with the Lewy body variant of Alzheimer’s disease and in those with Alzheimer’s disease alone, slightly more so in the caudate of the former.59 The metabolite of 5HT, 5 hydroxyindole acetic acid (5HIAA), is reduced in the superior and midtemporal gyri of patients with senile dementia of the Lewy body type, but the decrement is more substantial in patients who experience hallucinations.74
The ratio of the activity of 5HIAA to that of ChAT (5HIAA/ChAT) is also greater in hallucinating patients with senile dementia of the Lewy body type compared to nonhallucinating patients with the same disorder or controls.74 Evaluation of 5HT/5HIAA levels suggests a lower turnover of serotonin in hallucinating (2.0) patients than in nonhallucinating (2.9) patients with Lewy body disease.75
5HT type-2 (5HT-2) receptors have also been investigated autoradiographically in the superior and midtemporal gyri of patients with senile dementia of the Lewy body type.74 5HT-2 receptor binding was reduced in nonhallucinating patients with senile dementia of the Lewy body type compared to hallucinating patients with the same disorder or control subjects. The levels were not significantly different between the latter two groups.74
The distribution of 5HT-2 binding in the cortical layers of the superior and midtemporal gyri of patients with Alzheimer’s disease, Parkinson’s disease with and without dementia, and senile dementia of the Lewy body type with and without hallucinations was also analyzed autoradiographically. In this study the cortical zones were labeled A-F, where zone C loosely correlated to layer III and zone E with layer V. In patients with Alzheimer’s disease, 5HT-2 binding was reduced in zones B through E (layers II – V). There was no difference in 5HT-2 binding between patients with Parkinson’s disease and controls. In demented patients with Parkinson’s disease, 5HT-2 binding was reduced in zones B and F (layers II and VI). In patients with senile dementia of the Lewy body type without hallucinations, 5HT-2 binding was reduced only in zone B (layer II). In contrast, 5HT-2 binding was reduced in zones C-E (layers III-V) in patients with the same disorder who had hallucinations. The number of Lewy bodies, which occurred predominantly in the lower cortical layers (IV-VI), was equal in hallucinating and nonhallucinating patients with senile dementia of the Lewy body type.13 This finding suggests that serotonergic dysfunction may be involved with psychiatric disturbances in patients with Lewy body dementia. Based on the imaging data discussed earlier,43 it would be interesting to determine if similar changes related to serotonergic function occur in the primary visual cortex.
Pharmacological Features
In patients with cortical Lewy body pathology, levadopa may attenuate parkinsonian symptoms.11 Antiparkinsonian drugs, however, can precipitate delusions and hallucinations,31 which may be early symptoms of Lewy body disease. Individuals with Lewy body disease can also respond adversely to other pharmacologic agents. Low doses of neuroleptics administered to combat psychiatric disturbances in demented Lewy body disease patients produce disastrous results. These drugs exacerbate dementia and reduce the patient’s life expectancy as shown by increased mortality rates.48,66,67,69 Neuroleptic drugs can also increase parkinsonian symptoms in individuals with Lewy body disease.31
Patients suspected to have dementing Lewy body disease may respond to tacrine, an acetylcholinesterase inhibitor.60 Patients with pure diffuse Lewy body disease may also respond preferentially to acetylcholinesterase inhibitors.61,72 Tacrine may increase levels of acetylcholine, which may be severely depleted in patients with diffuse Lewy body disease.
Conclusions
Although the nomenclature of Lewy body disease continues to be controversial, the existence of Lewy body neuropathology assuredly plays an important role in precipitating psychiatric symptoms and eventually dementia in affected individuals. Visual hallucinations early in the clinical course differentiate dementing Lewy body disease from the next closest associated neurodegenerative disorders, Alzheimer’s disease and Parkinson’s disease. In these patients, extreme caution should be exercised when treating psychiatric symptoms with neuroleptic drugs, which can precipitate early death. There is still a paucity of investigations on Lewy body disease. Continued clinical, chemical, and neuropathological correlative studies of dementing Lewy body disease may provide the clues necessary to treat and perhaps eradicate this disorder.
References
- Albin RL, Minoshima S, D’Amato CJ, et al: Fluoro-deoxyglucose positron emission tomography in diffuse Lewy body disease.Neurology 47:462-466, 1996
- Antoine JC, Tommasi M, Chalumeau A, et al: Hallervorden-Spatz disease with Lewy bodies. Rev Neurol (Paris) 141:806-809, 1985
- Armstrong M, Daly AK, Cholerton S, et al: Mutant debrisoquine hydroxylation genes in Parkinson’s disease. Lancet 339:1017-1018, 1992
- Armstrong TP, Hansen LA, Salmon DP, et al: Rapidly progressive dementia in a patient with the Lewy body variant of Alzheimer’s disease. Neurology 41:1178-1180, 1991
- Ballard C, Patel A, Oyebode F, et al: Cognitive decline in patients with Alzheimer’s disease, vascular dementia and senile dementia of Lewy body type. Age Ageing 25:209-213, 1996
- Bergeron C, Pollanen M: Lewy bodies in Alzheimer’s disease—one or two diseases? Alzheimer Dis Assoc Disord 3:197-204, 1989
- Betard C, Robitaille Y, Gee M, et al: Apo E allele frequencies in Alzheimer’s disease, Lewy body dementia, Alzheimer’s disease with cerebrovascular disease and vascular dementia. Neuroreport 5:1893-1896, 1994
- Bhatia KP, Daniel SE, Marsden CD: Familial parkinsonism with depression: A clinicopathological study. Ann Neurol 34:842-847, 1993
- Bodhireddy S, Dickson DW, Mattiace L, et al: A case of Down’s syndrome with diffuse Lewy body disease and Alzheimer’s disease.Neurology 44:159-161, 1994
- Burkhardt CR, Filley CM, Kleinschmidt-DeMasters BK, et al: Diffuse Lewy body disease and progressive dementia. Neurology 38:1520-1528, 1988
- Byrne EJ, Lennox G, Lowe J, et al: Diffuse Lewy body disease: Clinical features in 15 cases. J Neurol Neurosurg Psychiatry 52:709-717, 1989
- Cercy SP, Bylsma FW: Lewy bodies and progressive dementia: A critical review and meta-analysis. J Int Neuropsychol Soc 3:179-194, 1997
- Cheng AV, Ferrier IN, Morris CM, et al: Cortical serotonin-S2 receptor binding in Lewy body dementia, Alzheimer’s and Parkinson’s diseases. J Neurol Sci 106:50-55, 1991
- Cornford ME, Chang L, Miller BL: The neuropathology of parkinsonism: An overview. Brain Cogn 28:321-341, 1995
- Crystal HA, Dickson DW, Lizardi JE, et al: Antemortem diagnosis of diffuse Lewy body disease. Neurology 40:1523-1528, 1990
- Dale GE, Probst A, Luthert P, et al: Relationships between Lewy bodies and pale bodies in Parkinson’s disease. Acta Neuropathol (Berl) 83:525-529, 1992
- de Vos RA, Jansen EN, Stam FC, et al: ‘Lewy body disease’: Clinico-pathological correlation in 18 consecutive cases of Parkinson’s disease with and without dementia. Clin Neurol Neurosurg 97:13-22, 1995
- Del-Ser T, Munoz DG, Hachinski V: Temporal pattern of cognitive decline and incontinence is different in Alzheimer’s disease and diffuse Lewy body disease. Neurology 46:682-686, 1996
- Dickson DW, Feany MB, Yen SH, et al: Cytoskeletal pathology in non-Alzheimer degenerative dementia: New lesions in diffuse Lewy body disease, Pick’s disease, and corticobasal degeneration. J Neural Transm Suppl 47:31-46, 1996
- Donnemiller E, Heilmann J, Wenning GK, et al: Brain perfusion scintigraphy with 99mTc-HMPAO or 99mTc-ECD and 123I-beta-CIT single-photon emission tomography in dementia of the Alzheimer-type and diffuse Lewy body disease. Eur J Nucl Med 24:320-325, 1997
- Duvoisin RC, Johnson WG: Hereditary Lewy-body parkinsonism and evidence for a genetic etiology of Parkinson’s disease. Brain Pathol 2:309-320, 1992
- Egensperger R, Bancher C, Kosel S, et al: The apolipoprotein E epsilon 4 allele in Parkinson’s disease with Alzheimer lesions.Biochem Biophys Res Commun 224:484-486, 1996
- Fearnley JM, Revesz T, Brooks DJ, et al: Diffuse Lewy body disease presenting with a supranuclear gaze palsy. J Neurol Neurosurg Psychiatry 54:159-161, 1991
- Forno LS: The Lewy body in Parkinson’s disease. Adv Neurol 45:35-43, 1987
- Forstl H, Burns A, Luthert P, et al: The Lewy-body variant of Alzheimer’s disease. Clinical and pathological findings. Br J Psychiatry 162:385-392, 1993
- Gai WP, Blumbergs PC, Blessing WW: Microtubule-associated protein 5 is a component of Lewy bodies and Lewy neurites in the brainstem and forebrain regions affected in Parkinson’s disease. Acta Neuropathol (Berl) 91:78-81, 1996
- Galasko D, Katzman R, Salmon DP, et al: Clinical and neuropathological findings in Lewy body dementias. Brain Cogn 31:166-175, 1996
- Galasko D, Saitoh T, Xia Y, et al: The apolipoprotein E allele epsilon 4 is overrepresented in patients with the Lewy body variant of Alzheimer’s disease. Neurology 44:1950-1951, 1994
- Galloway PG, Mulvihill P, Perry G: Filaments of Lewy bodies contain insoluble cytoskeletal elements. Am J Pathol 140:809-822, 1992
- Galvin JE, Lee VM, Baba M, et al: Monoclonal antibodies to purified cortical Lewy bodies recognize the mid-size neurofilament subunit. Ann Neurol 42:595-603, 1997
- Geroldi C, Frisoni GB, Bianchetti A, et al: Drug treatment in Lewy body dementia. Dement Geriatr Cogn Disord 8:188-197, 1997
- Gibb WR: Idiopathic Parkinson’s disease and the Lewy body disorders. Neuropathol Appl Neurobiol 12:223-234, 1986
- Gibb WR, Esiri MM, Lees AJ: Clinical and pathological features of diffuse cortical Lewy body disease (Lewy body dementia). Brain 110:1131-1153, 1987
- Gibb WR, Lees AJ: The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson’s disease. J Neurol Neurosurg Psychiatry 51:745-752, 1988
- Gibb WR, Scaravilli F, Michund J: Lewy bodies of subacute sclerosing panencephalitis. J Neurol Neurosurg Psychiatry 53:710-711, 1990
- Gibb WR, Scott T, Lees AJ: Neuronal inclusions of Parkinson’s disease. Mov Disord 6:2-11, 1991
- Hansen L, Salmon D, Galasko D, et al: The Lewy body variant of Alzheimer’s disease: A clinical and pathologic entity. Neurology 40:1-8, 1990
- Hansen LA, Galasko D, Samuel W, et al: Apolipoprotein-E epsilon-4 is associated with increased neurofibrillary pathology in the Lewy body variant of Alzheimer’s disease. Neurosci Lett 182:63-65, 1994
- Harrington CR, Louwagie J, Rossau R, et al: Influence of apolipoprotein E genotype on senile dementia of the Alzheimer and Lewy body types. Significance for etiological theories of Alzheimer’s disease. Am J Pathol 145:1472-1484, 1994
- Hayashi S, Akasaki Y, Morimura Y, et al: An autopsy case of late infantile and juvenile neuroaxonal dystrophy with diffuse Lewy bodies and neurofibrillary tangles. Clin Neuropathol 11:1-5, 1992
- Helisalmi S, Linnaranta K, Lehtovirta M, et al: Apolipoprotein E polymorphism in patients with different neurodegenerative disorders. Neurosci Lett 205:61-64, 1996
- Hely MA, Reid WG, Halliday GM, et al: Diffuse Lewy body disease: Clinical features in nine cases without coexistent Alzheimer’s disease. J Neurol Neurosurg Psychiatry 60:531-538, 1996
- Howard R, David A, Woodruff P, et al: Seeing visual hallucinations with functional magnetic resonance imaging. Dement Geriatr Cogn Disord 8:73-77, 1997