


Alternative Treatments for Intractable Epilepsy
Alan G. Stein, MD
Division of Neurology, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
Usually, epilepsy can be well treated with medications, surgery, or both. For the small percentage of patients who do not benefit from treatment with these modalities, alternative treatment strategies exist. Most of these alternative treatments have not undergone rigorous testing as have medications approved by the Food and Drug Administration. Evidence, however, still suggests that these alternative treatments are efficacious and safe. Such treatments include vagal nerve stimulation, the ketogenic diet, radiosurgery, and electroencephalographic biofeedback. Focal drug delivery and deep brain electrical stimulation are two promising experimental modalities that may someday prove effective.
Key Words: electrical stimulation, epilepsy, radiosurgery, vagus nerve
Epilepsy affects approximately 1% of the population. Most of these patients are effectively managed with the traditional medical or surgical treatments discussed elsewhere in this issue. For the minority of patients who cannot be made seizure free, however, alternative treatments exist or are in the process of being developed. This article provides an overview of the alternative treatments currently available or that show promise for future applicability to this difficult problem: the ketogenic diet, radiosurgery, vagal nerve stimulation, and biofeedback. Deep brain stimulation and focal drug delivery are two promising therapies still in the experimental stages of development.
The Ketogenic Diet
The positive effects of fasting on controlling seizures have been known since Biblical times (Mark 9:19-24). Unfortunately, the scientific rationale still eludes us, and fasting can only be maintained for a few days before starvation ensues. The ketogenic diet, however, is an extension of the metabolic state induced by fasting and can be maintained indefinitely. Before the advent of what is now considered modern antiepileptic drugs, the ketogenic diet was a topic of active research at a number of major medical centers.28 Until a recent flurry of publicity in the popular press brought it back into the mainstream of the epilepsy community, however, the ketogenic diet had lived in relative obscurity for the past 50 years.
This special diet consists of a very high proportion of fats compared with carbohydrates and proteins. The goal of the diet is to induce a prolonged state of ketosis, which, via unknown mechanisms, significantly reduces the frequency of seizures for a sizable proportion of patients placed on the diet. Speculation on the mechanism of action centers on the alteration in metabolism induced by the switch to a fatty acid-based energy source. The abnormal electroencephalogram (EEG) may normalize once the patient is on the diet. When carbohydrate intake is resumed, however, the EEG can quickly resume an epileptiform appearance.11
The true efficacy of the ketogenic diet is difficult to ascertain for two reasons. Because the diet is markedly different from a normal diet and difficult to administer, blinded studies are infeasible and randomized studies have not been performed. And because the diet is difficult to maintain, patients who do not have a positive response tend to discontinue it quite early. Consequently, outcomes in terms of efficacy tend to be skewed because the population who continues a treatment tend to be those who are clinical responders.
Looking at an intent-to-treat population, however, suggests that the ketogenic diet may be as efficacious as drug treatment and also may allow patients to reduce their number of medications. The Johns Hopkins center reported that of 150 patients who started the diet, 44% experienced a 50% or greater reduction in their seizures after 1 year and 50% of all patients stayed on the diet for 1 year or longer.9 In a prior study, 64% of patients were able to reduce their antiepileptic drugs.12 About 10% of all patients started on the diet were able to discontinue medications altogether. The major side effect of the diet is diarrhea or constipation, but a few more serious complications have been reported.2
Induction and maintenance of the ketotic state are not easy tasks. Typically, ketosis is induced by having patients fast until their urine demonstrates significant ketone bodies (approximately 24 hours). The ketogenic diet is then gradually introduced over the next 2 days. The degree of ketosis is easily monitored by standard urine reagent test strips, which show ketones. Once ketosis has been achieved, strict adherence to the diet must be maintained or the body will revert back to glucose-based metabolism.
The diet is composed of a rather rigid ratio of high fat-to-low protein and carbohydrates. The optimal ratio is debated but is usually considered to range between 3:1 and 4:1.22 These are weight-based ratios, which translate into a percentage of calories from fat of almost 90% (in the case of the 4:1 ratio diet). Obesity is avoided by careful control of total daily caloric intake. The patient’s total daily caloric and protein requirements are assessed based on body size. Once these requirements are determined, the amount of allowable carbohydrates can easily be calculated.
Most centers start patients on the diet on an inpatient basis and use a nutritionist. The role of the nutritionist should not be underestimated, especially in helping families to learn about what foods can and cannot be eaten on the diet. Easily overlooked sources of excess carbohydrates are the filler ingredients in medications, especially in oral suspensions and children’s chewable tablets.7
Radiosurgery
The very focal application of radiation is a relatively new treatment for focal brain lesions, especially for tumors or vascular malformations. The technique relies upon highly focused ionizing radiation to create a precise area of tissue injury. Radiosurgery can be performed with one of two devices, the LINAC or the Gamma Knife, which jointly are referred to as radiosurgery devices. In the 1950s, early attempts at developing radiosurgery devices were limited by the large size of linear accelerators. The current LINAC overcomes this obstacle. Available in the United States since 1987, the Gamma Knife in its current form consists of 201 cobalt radiation sources (60 Co) that emit finely focused beams of gamma radiation. The Gamma Knife operates by coalescing these 201 beams onto a very small focus. The LINAC, although very different in design, likewise focuses a high-intensity beam of radiation onto a small area.
Because of the focusing effect of radiosurgery devices, the epicenter of radiation receives a large, intense dose of ionizing gamma radiation while the surrounding tissue receives a much smaller dose. Moving away from the epicenter, radiation exposure decreases by the cube of the distance. Dosimetry can be calculated to create a necrotizing dose at the epicenter. By limiting the radiation, a subnecrotizing dose can be used. The procedure is noninvasive and can be performed in a single setting. It has very few immediate side effects, and the intermediate and long-term side effects do not manifest until the affected tissue attempts replication. In the brain, with its slowly dividing tissues, the effects are not seen for several weeks to months at which time they often can be visualized on magnetic resonance (MR) imaging. Tissue may be functionally impaired before the changes on MR imaging are visible. If necrotizing doses are used, significant focal edema may develop. Rare side effects are hydrocephalus or stroke caused by radiation-induced angiopathy.16
The reduction of seizures after radiosurgery has been evaluated in a few instances. Most positive data come from the treatment of arteriovenous malformations (AVMs) where a significant number of patients have become seizure free. Seizure reduction was not studied as a primary endpoint in these studies, and detailed data regarding the frequency and severity of seizures before and after radiosurgical treatment are unavailable. In these cases, seizure reduction may reflect either direct injury from radiation of the epileptic cortex in the area, tissue dysfunction from the reduced blood flow after ablation of the AVM, or disruption of the propagation pathways of the seizure rather than the seizure focus itself.
The use of radiosurgery specifically to reduce seizures has been investigated in a few pilot studies and is reviewed elsewhere.4 These studies used necrotizing doses of radiation to deliver functional amygdalohippocampectomies to treat mesial temporal sclerosis19 and focal lesions and to perform functional corpus callosotomies in patients with intractable atonic seizures.6 Short-term results in the groups undergoing amygdalohippocampectomies and the corpus callosotomies have been promising, but long-term follow-up was limited to less than 16 months at the time of reporting. Several patients developed significant edema.
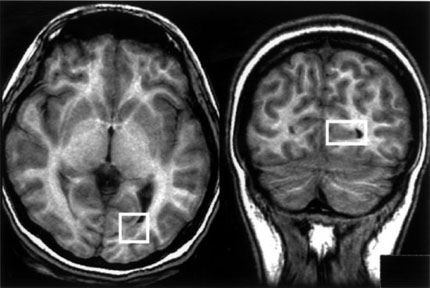
More likely candidates for radiosurgery are patients with small, deeply seated lesions that would be difficult to excise safely using standard surgical procedures (Fig. 1). Whang and Kwon27 reported the long-term follow-up (longer than 1 year) of 23 patients with focal lesions causing partial seizures—mostly partial complex seizures with secondary generalization. The duration of seizures before radiosurgery ranged from 1 to 25 years, and all 23 patients had failed multiple medical treatments. The diameter of all lesions was less than 2.0 cm, and they remained stable on diagnostic imaging over a 6-month period. The results 6 months after radiosurgery were disappointing, however. Only three patients were free of seizures (Engel Class I). At the 12-month follow-up, nine (39%) patients were free of seizures. By the end of the study (mean follow-up, 37 months), 12 patients (52%) were seizure free. Two patients developed asymptomatic perioperative edema seen on diagnostic imaging, and no patients developed new deficits.
The efficacy for the long-term control of seizures is still unknown as are the long-term effects of this type of ionizing radiation exposure. As these questions are answered, however, radiosurgery may emerge as an excellent technique for delivering relatively noninvasive treatment of intractable focal seizures, especially those caused by discrete lesions not safely accessed by standard surgical techniques.
Vagal Nerve Stimulator
The vagal nerve stimulator, a new device for the treatment of intractable partial epilepsy, was approved by the Food and Drug Administration in 1997. A truly novel approach to seizure control, the vagal nerve stimulator is a development that dates to the 1950s. Early animal studies showed that stimulation of the vagus nerve affects cortical potentials, including evoked potentials and EEG. Depending upon the type of stimulation given, the EEG pattern became more or less synchronized. In 1952 it was found that vagal nerve stimulation could block interictal spiking from a strychnine focus, and seizures have actually been aborted and prevented in a variety of animal models of epilepsy.20 The first limited trial with an implanted device in humans showed promising results in a small number of subjects. Larger randomized trials testing high- and low-intensity stimulation confirmed that the vagal nerve stimulator had a positive effect on seizure control.25
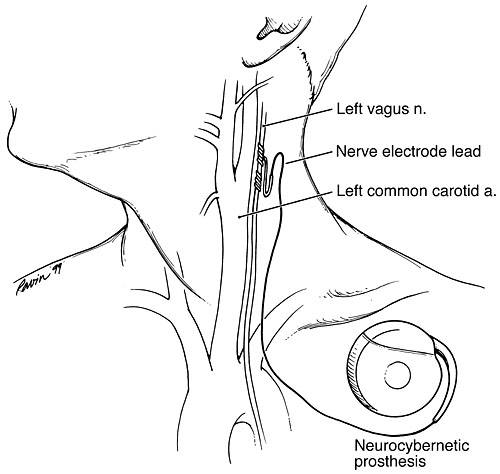
The vagal nerve stimulator unit looks much like a cardiac pacemaker. It consists of a round stimulator unit with an attached stimulator wire. The unit is implanted surgically by attaching the anode, cathode, and ground electrodes to the left vagus nerve just deep to the carotid artery (Fig. 2). The stimulating wires are then tunneled to the stimulation unit, which is implanted in a subcutaneous pocket created in the infraclavicular area on the left side.
Although the vagus nerve has widespread input to multiple organs, its effect on gastric secretion or cardiac rhythm appears to be little if any. The left vagus nerve is used because it has fewer fibers connecting with cardiac pacemakers. Stimulation parameters are fully adjustable, but the standard rate of stimulation is 30 seconds of “on” stimulation followed by 5 minutes of no stimulation. The unit has a magnetic sensor so if the patient or family holds a strong magnet (supplied to the patient on a wristband) to the device, it can be activated manually. The parameters of manual activation are also fully adjustable but typically are set at a level that is more intense than baseline.
The vagus nerve transmits a large number of input signals from visceral afferents that terminate in the nucleus solitarius in the medulla. Presumably, vagal nerve stimulation is able to influence EEG patterns through subcortical connections via the thalamus. Variations in parameters such as stimulation intensity or repetition rate affect the EEG differently. Some of these effects are caused by stimulation of different vagal afferent fibers (unmyelinated versus larger myelinated fibers) while others may reflect stimulation frequencies. Actually, the exact mechanisms of the antiepileptic effect of vagal nerve stimulation are unclear. Repetitive painful stimulation of a rat’s tail produces a greater anticonvulsive effect than does vagal nerve stimulation. This finding raises the question of whether the antiseizure effect reflects little more than a general alerting response.
The efficacy of vagal nerve stimulation is similar to most of the newly introduced antiepileptic drugs: the frequency of seizures in about 30% of patients is reduced 50% or more.18 Several features of the response to the vagal nerve stimulator are interesting, however. First, the degree of seizure reduction increases with the length of time the patient wears the vagal nerve stimulator. Responses at 3 months averaged a 20% decrease in seizure frequency whereas the effect had risen to 32% by 12 months (a statistically significant change).21 This finding contrasts with most clinicians’ experience of placing patients on new medications. After a honeymoon period, the frequency of seizures usually returns to its prior level within a few months.
The other exciting finding about the vagal nerve stimulator is some patients’ ability to abort their seizures by activating their stimulating unit manually. Pellagi and Morris15 found that approximately 20% of patients could abort their seizures. Another 35% of patients reported that their seizures were “lighter” after manual activation of the vagal nerve stimulator during a seizure. Despite these advantages, no patients became free of seizures during the blind phase of either large-scale randomized study.
Side effects from the vagal nerve stimulator are mostly mild and easily tolerated. Common adverse reactions are a sense of tingling or discomfort in the neck and a hoarseness of the voice during stimulation. During the clinical trials, one patient sustained permanent injury to the left vagal nerve because the equipment malfunctioned and electrical stimulation continued.18 Another patient had a non-Q wave myocardial infarction, but it was unclear if the episode was related to the stimulation. There appears to be no significant increase in unexplained sudden deaths in patients using the vagal nerve stimulator compared to the number of deaths in equivalent patients with severe epilepsy.1
Biofeedback
Biofeedback is a unique approach to epilepsy control. External stimuli can affect many seizures either positively or negatively. Examples of seizures triggered by external stimuli are reflexive epilepsy and reading epilepsy. Some individuals can abort their seizure by vigorously stimulating a limb at the time of onset. As described above, the severity of a seizure can sometimes be modified by manual activation of the vagal nerve stimulator. Presumably, the seizure activity in all these cases is modified because the peripheral stimulation alters underlying brain wave patterns and organization. With appropriate feedback mechanisms, some individuals can learn to modify their brain wave pattern simply by “thinking” in a certain way. It therefore may be possible to manipulate brain wave patterns in such as way as to reduce the likelihood of seizures.
In the late 1960s, animal research demonstrated that some species could alter their cortical EEG activity when given the appropriate reinforcing feedback. Animals in which enhanced sensorimotor 12 to 16 Hz activity was reinforced were more resistant to chemically induced seizures than untrained animals or animals trained to suppress this cortical activity. In the early 1970s, a number of articles reported that patients with intractable epilepsy could be similarly trained to enhance specific “sensorimotor activity” with variable degrees of seizure control.
The efficacy of biofeedback control of seizures has been controversial. Early published reports showed response rates of 60 to 75%. In these patients, the average reduction in seizures was as high as 74%.13,24 Quy and colleagues17 even reported 100% of patients responding positively, but the sample consisted of only three patients.17 All of these studies, in fact, relied on relatively small numbers of patients. Consequently, results have been received less than enthusiastically.
Wyler and coworkers29 studied 23 patients trained in a slightly different paradigm. Approximately 50% of the patients “had a significant reduction in seizure frequency.” Despite the objective decrease in seizure frequency, however, not all patients noted a subjective improvement in their life. Sterman and Macdonald24 found a continued reduction in seizures even at a 6-month follow-up, but Wyler et al.29 found that many patients rapidly reverted to their baseline frequency when EEG biofeedback was discontinued. They concluded that EEG biofeedback was not cost effective for most patients. Their paradigm, however, which incorporated more intensive training for a far briefer period compared to other studies, may be responsible for the difference.
The method used by Sterman and Macdonald,24 Wyler et al.,29 and most other centers provided a reward for enhanced “good” activity and a negative reward for “bad” activity. During production with artifact and high-voltage activity, feedback ceased. Cott and coworkers3 suggested that the high-voltage “time out” activity could represent epileptiform activity, and the cessation of feedback could represent a “punishment” for epileptiform activity. They found that feedback paradigms with negative reinforcement only during such time-out periods changed the frequency of seizures as much as the traditional approach. Sterman and Macdonald,24 however, later refuted this assertion.
Despite markedly lowered costs and significant improvements in computerized EEG processing equipment, the literature regarding biofeedback control of seizures has been silent the past 15 to 20 years. As a means of seizure control, EEG biofeedback has more or less fallen from favor. Few, if any, centers actively promote its use. Perhaps it is time to revisit this therapeutic modality.
Focal Drug Delivery
For most patients with intractable epilepsy, their seizures start in a focal area and then spread. Complete removal of the area of seizure onset effectively cures the epilepsy. The aim of seizure surgery is exactly complete removal of the epileptic zone. Unfortunately, this goal cannot be achieved safely if the zone of onset is in eloquent cortex or if there are multiple foci. For such patients, the current options of therapeutic intervention are limited.
One approach under investigation is the direct delivery of anticonvulsant medication to the seizure focus rather than through the systemic circulation. The advantages of this approach are quite straightforward. Systemic side effects are limited. High concentrations of an anticonvulsant drug can be delivered locally. If linked to a seizure-detection or manual-stimulation module, the toxic therapeutics can be delivered only when the seizure occurs.
A number of delivery devices for the focal application of central nervous system active drugs already exist. These devices include intrathecal pumps for the delivery of antispasticity agents, reservoir systems for the delivery of antineoplastic agents, and implanted wafer systems for the slow release of antineoplastic agents. Other methods of localized drug delivery are also under investigation.
The application of these technologies toward the treatment of epilepsy has been progressing in recent years. R.J. Tamargo (personal communication, 1998) applied a degradable polymer matrix wafer containing phenytoin to an experimental seizure focus in the rat and demonstrated reduction in the severity scores of both behavioral and EEG seizure activity. Smith et al.23 injected lidocaine into a bicuculline epileptic focus thereby causing clinically apparent seizure activity to cease.23 Eder and coworkers 4,5 injected a more traditional anticonvulsant drug, diazepam, into epileptic foci created by a variety of models. Focal diazepam markedly reduced interictal spiking in all of these models. A later adaptation of this model included the integration of a computerized seizure-detection algorithm to trigger injection of the drug only at seizure onset.
Thus far, the results of such studies have been promising, but considerable work remains to be done. Equipment needs further miniaturization. Computerized seizure-detection programs must improve. Finally, safety profiles for these approaches must be established before they can become clinically useful tools.
Deep Brain Stimulation
Similar to focal application of an anticonvulsant drug, it may be possible to stop or suppress seizures by focal electrical stimulation within the epileptic focus itself or within a modulating pathway. Velasco et al.26 stimulated the parahippocampal gyrus in a small number of patients with intractable partial complex seizures of mesial temporal origin. Stimulation ipsilateral to the focus completely abolished all clinical and EEG seizure activity during the 3 to 4 days of stimulation. Whether continued stimulation would have similar long-term effects is unknown.
As discussed above, the vagal nerve stimulator is thought to exert its effect via subcortical pathways that presumably synapse in the thalamus. Henry and colleagues10 found that positron emission tomography activation of one or both thalami during acute vagal nerve stimulation predicted the individual’s response to the stimulation. Earlier work in animals had also shown that thalamic stimulation influenced seizures. Mirski and coworkers14 found that high-frequency (100 Hz) stimulation of the anterior thalamus in the rat raised the seizure threshold while low-frequency stimulation (8 Hz) lowered the seizure threshold. One attempt at a controlled trial in humans failed to find statistical significance although one patient did respond dramatically. This patient, however, could not be included in the analysis because she did not enter the placebo phase of the study.8
Summary
For patients who cannot be treated effectively with standard therapies, alternative treatments exist. With the exception of the vagal nerve stimulator, these treatment modalities have not been tested rigorously. Notwithstanding, these treatment strategies should still be considered for the small percentage of patients for whom there is little other hope. In the future, other methods of treatment may become available.
References
- Annegers JF, Coan SP, Hauser WA, et al: Epilepsy, vagal nerve stimulation by the NCP system, mortality, and sudden, unexpected, unexplained death. Epilepsia 39:206-212, 1998
- Ballaban-Gil K, Callahan C, O’Dell C, et al: Complications of the ketogenic diet. Epilepsia 39:744-748, 1998
- Cott A, Pavloski RP, Black AH: Reducing epileptic seizures through operant conditioning of central nervous system activity: Procedural variables. Science 203:73-75, 1979
- Eder HG, Fisher RS: The role of the Gamma Knife in the treatment of seizures. BNI Quarterly 13:37-40, 1997
- Eder HG, Jones DB, Fisher RS: Localized epidural perfusion of diazepam attenuates epileptiform activity in the rat bicuculline model of epilepsy. Epilepsia 37:67, 1996
- Eder HG, Schröttner O, Pendl G: Radiochirurgische kallosotomie bei epilepsie (abstract). Zentralbl Neurochir 5(Suppl):16, 1996
- Feldstein TJ: Carbohydrate and alcohol content of 200 oral liquid medications for use in patients receiving ketogenic diets. Pediatrics 97:506-511, 1996
- Fisher RS, Uematsu S, Krauss GL, et al: Placebo-controlled pilot study of centromedian thalamic stimulation in treatment of intractable seizures. Epilepsia 33:841-851, 1992
- Freeman JM, Vining EPG, Swink TD, et al: Effectiveness of the ketogenic diet in difficult-to-control seizures: 150 consecutive cases followed up more than 6 months. Epilepsia 38:194, 1997
- Henry TR, Dunwoody GA, Votaw JR, et al: Therapeutic response correlates with thalamic blood flow increases induced acutely by vagus nerve stimulation in partial epilepsy. Neurology 50:66, 1998
- Huttenlocher PR: Ketonemia and seizures: Metabolic and anticonvulsant effects of two ketogenic diets in childhood epilepsy. Pediatr Res 10:536-540, 1976
- Kinsman SL, Vining EP, Quaskey SA, et al: Efficacy of the ketogenic diet for intractable seizure disorders: Review of 58 cases. Epilepsia 33:1132-1136, 1992
- Kuhlman WN: EEG feedback training of epileptic patients: Clinical and electroencephalographic analysis. Electroencephalogr Clin Neurophysiol 45:699-710, 1978
- Mirski MA, Rossell LA, Terry JB, et al: Anticonvulsant effect of anterior thalamic high frequency electrical stimulation in the rat. Epilepsy Res 28:89-100, 1997
- Pellagi J, Morris G, Vagus Nerve Group: The efficacy of hand-held magnetic activation of vagal nerve stimulation in refractory epilepsy patients. Neurology 50:A201, 1998
- Park YG, Chung SS, Kim DI, et al: Complications following Gamma Knife radiosurgery. Stereotact Funct Neurosurg 64:239-248, 1995
- Quy RJ, Hutt SJ, Forrest S: Sensorimotor rhythm feedback training and epilepsy: Some methodological and conceptual issues. Biol Psychol 9:129-149, 1979
- Ramsay RE, Uthman BM, Augustinsson LE, et al: Vagus nerve stimulation for treatment of partial seizures: 2. Safety, side effects, and tolerability. First International Vagus Nerve Stimulation Study Group. Epilepsia 35:627-636, 1994
- Regis J, Peragui JC, Rey M, et al: First selective amygdalohippocampal radiosurgery for ‘mesial temporal lobe epilepsy’. Stereotact Funct Neurosurg 64:193-201, 1995
- Rutecki P: Anatomical, physiological, and theoretical basis for the antiepileptic effects of vagus nerve stimulation. Epilepsia 31:1-6, 1990
- Salinsky MC, Uthman BM, Ristanovic RK, et al: Vagus nerve stimulation for the treatment of medically intractable seizures. Results of a 1-year open-extension trial. Vagus Nerve Stimulation Study Group. Arch Neurol 53:1176-1180, 1996
- Schwartz RH, Eaton J, Bower BD, et al: Ketogenic diets in the treatment of epilepsy: Short-term clinical effects. Dev Med Child Neurol 31:145-151, 1989
- Smith DC, Krahl SE, Browning RA, et al: Rapid cessation of focally induced generalized seizures in rats through microinfusion of lidocaine hydrochloride into the focus. Epilepsia 34:43-53, 1993
- Sterman MB, Macdonald LR: Effects of central cortical EEG feedback training on incidence of poorly controlled seizures. Epilepsia 19:207-222, 1978
- The Vagus Nerve Stimulation Study Group: A randomized controlled trial of chronic vagus nerve stimulation for treatment of medically intractable seizures. Neurology 45:224-230, 1995
- Velasco M, Velasco F, Velasco AL: Effect of long-term electrical stimulation of the hippocampal gyrus on intractable temporal-lobe seizures. Epilepsia 38:71, 1997
- Whang CJ, Kwon Y: Long-term follow-up of stereotactic Gamma Knife radiosurgery in epilepsy. Stereotact Funct Neurosurg 66:349-356, 1996
- Wheless JW: The ketogenic diet: Fa(c)t or fiction. J Child Neurol 10:419-423, 1995
- Wyler AR, Robbins CA, Dodrill CB: EEG operant conditioning for control of epilepsy. Epilepsia 20:279-286, 1979