


Dolichoectatic Basilar Artery Aneurysm Treated with Superficial Temporal Artery-to-Superior Cerebellar Artery Bypass and Coiling: Case Report
A. Giancarlo Vishteh, MD†
Cargill H. Alleyne, Jr., MD‡
Cameron G. McDougall, MD
Robert F. Spetzler, MD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Current Address: †Quantum Neurological Surgery, Phoenix, Arizona,
‡Department of Neurosurgery, University of Rochester, Rochester, New York
Abstract
Despite advances in endovascular and microsurgical techniques, the treatment of giant aneurysms of the basilar apex can still lead to significant morbidity and mortality. We present a 54-year-old female with signs and symptoms of brain stem compression. Evaluation revealed a giant calcific, fusiform aneurysm of the basilar artery. The aneurysmal inflow channel arose along the basilar apex and the outflow ended in the superior cerebellar artery. Because of the complexity of this lesion, she had been deemed inoperable at other centers and was referred to our institution. She underwent a superficial temporal artery-to-superior cerebellar artery bypass followed by coil occlusion of the aneurysmal channel. She did well and was discharged home 5 days later. The management paradigm for this complex aneurysm is detailed.
Key Words: aneurysms, bypass, dolichoectatic
Aneurysms of the basilar apex are the most common aneurysms of the posterior circulation. Surgical or endovascular treatment of giant saccular aneurysms at this locale, however, can be associated with significant morbidity and mortality rates because of the proximity of vital neural structures, the potential of injuring perforating arteries, and the technical difficulties of obliterating such aneurysms completely. A subset of these aneurysms, the so-called fusiform aneurysms, are even more complex because of their inflow and outflow sites, and they represent an even greater challenge to neurovascular surgeons. For such rare and complex cases, an individualized combination of endovascular and surgical approaches may help obtain optimal clinical results in deteriorating patients.
Case Report
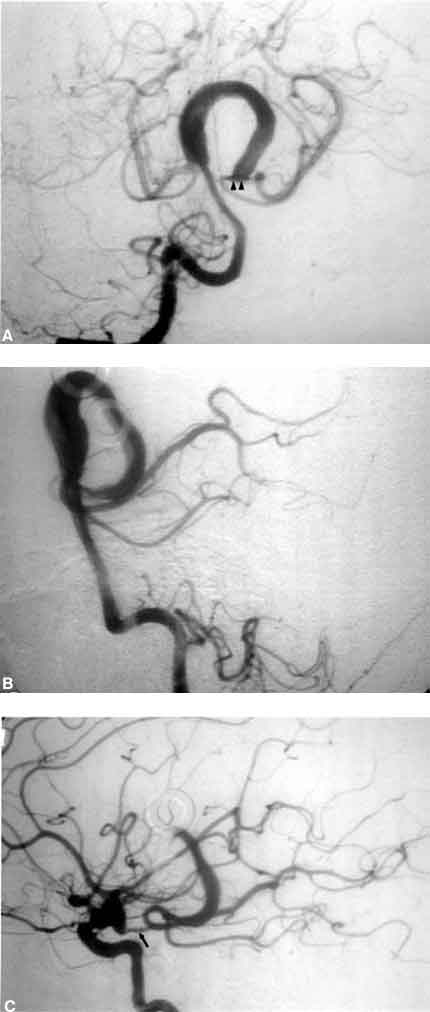
A 54-year-old female came to medical attention with diplopia and signs and symptoms of brain stem compression. Partial third nerve paresis and long tract signs were noted on examination. Computed tomography and magnetic resonance imaging were consistent with the diagnosis of a giant thrombosed aneurysm of the basilar terminus. Angiography revealed an aneurysmal mass with a large central thrombotic component and a channel that involved the origin and P1 segment of the posterior cerebral artery (PCA) and appeared to end at the origin of the left superior cerebellar artery (Fig. 1A and B). The patient’s left posterior communicating artery (PCoA) appeared intact (Fig. 1C). The complex aneurysm itself was deemed unamenable for direct clipping or clip reconstruction of the parent vessel. A multidisciplinary treatment strategy involving the irrigation of the distribution of the superior cerebellar artery (via a bypass) followed by endovascular occlusion of the aneurysmal channel was therefore planned.
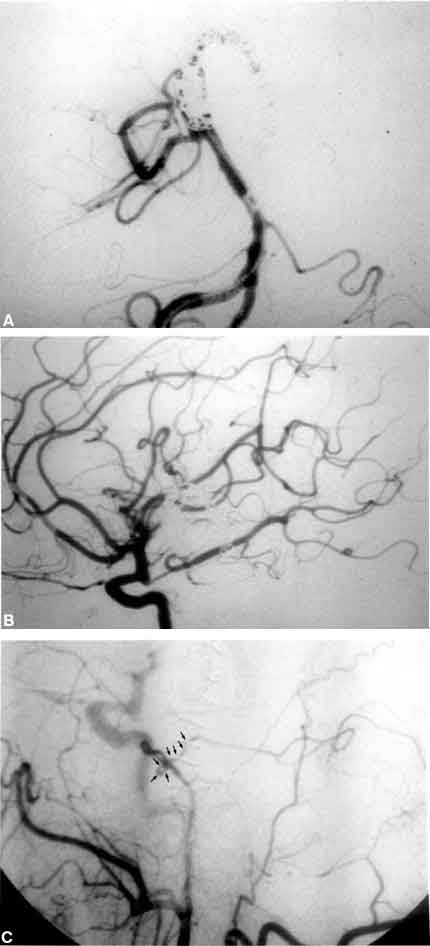
The patient underwent a left pterional craniotomy with orbitozygomatic osteotomies. A preserved frontal branch of the superficial temporal artery was anastomosed end-to-side to the left superior cerebellar artery using two 10-0 monofilament sutures (under barbiturate suppression). The patient tolerated the procedure well and 2 days after surgery underwent angiography, which documented the patency of the bypass graft. During the same angiographic session, she underwent coil occlusion of the aneurysm channel at the level of the P1 segment of the PCA (Fig. 2A). As noted on angiography and intraoperatively, the patient’s PCoA was patent, permitting coil occlusion of the aneurysmal channel. Angiography of the left internal carotid artery after coiling revealed filling of the P2 and distal segments of the PCA via the ipsilateral PCoA (Fig. 2B). Patency of the superior temporal artery-to-superior cerebellar artery bypass graft (Fig. 2C) was established by an angiographic injection of the left external carotid artery.
After a short course of postoperative anticoagulation therapy (heparin), the patient was placed on antiplatelet therapy and discharged home 5 days after surgery in stable condition. At a 6-month follow-up examination, the patient continued to do well. Her diplopia had significantly improved to the point where she was able to drive a car.
Discussion
Fusiform aneurysms of the vertebrobasilar system are formidable surgical challenges. Patients suffering from thrombo-embolism from the aneurysm nidus are usually treated with anticoagulation and/or antiplatelet therapy. In patients who are symptomatic from mass effect, however, treatment has involved Hunterian ligation of the parent vessels (mostly as a temporizing measure). In patients with complex fusiform aneurysms of the basilar artery, this approach ultimately led to sacrifice of one or both vertebral arteries. If the patient tolerated the parent vessel occlusion acutely, collateralization of blood flow led to continued growth of the aneurysm and the patient’s eventual death.
As bypass techniques and endovascular therapy have evolved, a number of these lesions have become amenable to multimodality treatment. This combination usually entails endovascular occlusion of the proximal parent vessel followed by distal bypass, where possible. Such labor-intensive surgeries, however, should be reserved for patients with the appropriate medical reserve. Furthermore, the trapping and bypass scheme must be individualized for each patient. In the present case, patency of the ipsilateral PCoA allowed coil occlusion of P1, and irrigation of the territory of the superior cerebellar artery was established via the pedicle bypass from the superior temporal artery.