


Cranial Application of Frameless Stereotaxy
Authors
G. Michael Lemole, Jr., MD
Jeffrey S. Henn, MD
Howard A. Riina, MD
Robert F. Spetzler, MD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
Frameless stereotaxy is uniquely suited to intracranial surgery. The relatively fixed position of the brain within the skull facilitates the referencing of preoperative data with the real-time position of the head. Frameless stereotaxy can be useful at all operative stages including selecting an approach, placing a craniotomy, and determining trajectories through or around cerebral structures. In particular, frameless stereotaxy has been applied successfully to vascular and neoplastic pathologies and to functional neurosurgery. As computing power, referencing techniques, and neuroimaging modalities advance, so too will the application of frameless stereotaxy in intracranial surgery.
Key Words: cranial, frameless stereotaxy
Neurosurgeons have long understood the complications associated with blind exploration through eloquent brain structures. Even the slightest variance from a planned trajectory to a lesion can be disastrous. To avoid these consequences, stereotactic guidance systems, including frameless stereotaxy, have been developed and are now common neurosurgical adjuncts. Proven useful for cranial surgery, frameless stereotaxy offers real-time imaging superimposed upon a data set obtained preoperatively. This information helps neurosurgeons to select an appropriate approach and to minimize its invasiveness. Intracranial targets can be localized and optimal trajectories chosen, thereby reducing the complications associated with excessive exposure, retraction, or violation of eloquent cerebral structures. Once a target such as a tumor is reached, frameless stereotaxy can help measure the dimensions of the lesion and guide the degree of resection. If hardware is to be inserted, frameless stereotaxy can help place it precisely.
Although frameless stereotaxy may be applied to various anatomical locations, the technique is most applicable to intracranial surgery because the cranium and its contents are relatively fixed. This relationship is not affected significantly by normal cardiac or respiratory variations. Consequently, preoperative imaging data can be closely correlated to intraoperative anatomy by referencing through a registration process. Frameless stereotaxy is invaluable at all stages of surgery, including selection of the preoperative approach, sizing of the scalp incision, placement of the craniotomy, and selection of the trajectory through or around cerebral structures. It is particularly suited to surgical treatment of neoplastic and vascular pathologies and functional applications. Frameless stereotaxy is intrinsically linked to advances in neuroimaging. In particular, the use of functional imaging in frameless stereotaxy represents an exciting opportunity for neurosurgeons to identify both anatomical structures and functional centers with great precision.
Development of Stereotactic Guidance
Although the mathematical and anatomical bases for frameless stereotaxy have existed for hundreds of years, frameless stereotaxy has only become a surgical reality in the last decade. Early attempts at localizing deep brain structures based on anatomical skull features can be traced to Leonardo da Vinci.[13] Horsley and Clarke,[12] however, constructed the first true stereotactic instrument by conceptualizing the relationship of skull landmarks and deep brain structures within a Cartesian coordinate system. This work was guided entirely by anatomical atlases of the brain and did not consider individual variability.[13] With the development of the stereoencephalotome in the 1940s by Spiegel et al.,[23] individual cranial landmarks could be referenced to stereotactic guidance systems. Subsequent refinements resulted in the use of arc-based stereotactic frames such as that designed by Leksell[16] in 1949. The advent of computed tomography (CT) and magnetic resonance (MR) imaging systems allowed more precise definition of intracranial structures; any intracranial structure could be localized using existing frame-based stereotactic systems.
As computing power increased in the 1980s, it logically followed that stereotactic localization could depart from frame-based systems while retaining the inherent accuracy of a Cartesian coordinate system. In 1986 Roberts first coined the term “frameless stereotaxy.”[19] Since then numerous devices have been designed to image, reference, and localize intracranial structures using the principles of frameless stereotaxy. These devices use preoperative image data sets as their reference upon which real-time localizer probe information is superimposed. Like frame-based systems, these systems share the same principles of referencing intracranial structures to an externally imposed Cartesian coordinate system.
Types of Stereotactic Systems
Naturally, any theoretical advantages gained by frameless stereotaxy must be weighed against its potential disadvantages. The latter include the learning curve associated with new technologies. Additional time may be required for preoperative setup. Space must be provided for the frameless stereotactic system within the operative theater. Some systems prove cumbersome within the surgical field. The individual advantages and disadvantages of the available frameless stereotactic systems vary and must be weighed against surgeons’ need for precision, accuracy, localization, and the overall integration of the frameless stereotactic system into the operating room (OR) setting.
Most frameless stereotactic systems consist of four major components: the stereotactic localizer or wand, the tracking system that measures the movement of the wand in space, the hardware system represented by the central processing unit (CPU) and monitor, and the software that converts all analog inputs regarding position into two- and three-dimensional spatial reconstructions. Differences between available systems include the tools with which a lesion is localized, the technology by which the localizing wand is triangulated, and the various display features available.
Types of Stereotactic Systems
Naturally, any theoretical advantages gained by frameless stereotaxy must be weighed against its potential disadvantages. The latter include the learning curve associated with new technologies. Additional time may be required for preoperative setup. Space must be provided for the frameless stereotactic system within the operative theater. Some systems prove cumbersome within the surgical field. The individual advantages and disadvantages of the available frameless stereotactic systems vary and must be weighed against surgeons’ need for precision, accuracy, localization, and the overall integration of the frameless stereotactic system into the operating room (OR) setting.
Most frameless stereotactic systems consist of four major components: the stereotactic localizer or wand, the tracking system that measures the movement of the wand in space, the hardware system represented by the central processing unit (CPU) and monitor, and the software that converts all analog inputs regarding position into two- and three-dimensional spatial reconstructions. Differences between available systems include the tools with which a lesion is localized, the technology by which the localizing wand is triangulated, and the various display features available.
One of the earliest technologies used to localize a point in space consisted of an articulated arm.[5,15,17,18,21,24] The ISG Wand frameless stereotactic guidance system (ISG Technologies, Mississauga, Ontario, Canada) is an excellent example. The localizer consists of a sterile surgical probe connected to a multi jointed, articulated arm with free movement in six directions. The information regarding joint position is sent to the computer where the analog data are converted into a digital format and correlated with the preexisting MR imaging data set. The accuracy of this technology is excellent; the range of error is 1 to 2 mm. The disadvantage of this system includes the inherent bulkiness of the articulated arm and its tendency to obstruct the operative field, especially when the microscope is employed, or when working down a narrow operative corridor.
One of the earliest technologies used to localize a point in space consisted of an articulated arm.[5,15,17,18,21,24] The ISG Wand frameless stereotactic guidance system (ISG Technologies, Mississauga, Ontario, Canada) is an excellent example. The localizer consists of a sterile surgical probe connected to a multi jointed, articulated arm with free movement in six directions. The information regarding joint position is sent to the computer where the analog data are converted into a digital format and correlated with the preexisting MR imaging data set. The accuracy of this technology is excellent; the range of error is 1 to 2 mm. The disadvantage of this system includes the inherent bulkiness of the articulated arm and its tendency to obstruct the operative field, especially when the microscope is employed, or when working down a narrow operative corridor.
To reduce the physical profile of the wand localizer, other technologies use arrays of ultrasonic emitters attached to the localizing wand and head-fixation system.[2-4] Signals produced by these emitters are received by a microphone array, and the data are then processed in the usual manner by the CPU. Most studies using this technology note average errors in localization of less than 4 mm. The localizing wands can be made to be very low profile. In fact, emitter arrays have been designed for use on a variety of neurosurgical instruments such as microsuckers and endoscopes, thereby converting the instruments into stereotactic localizers. Ultrasonography, however, is subject to considerable ambient interference. The reliability of triangulation using sound depends on air temperature and the presence of air currents within the OR. Furthermore, any instrument that produces ultrasonic noise itself (e.g., microsuckers) can decrease the accuracy of localization.

To capitalize on the advantages of a lower profile wand while avoiding the complications of using ultrasound, some systems have replaced sound emitters with light-emitting diodes (LEDs).[7,11,20] The LEDs are placed along the localizing instruments, and their signal is triangulated by a series of infrared camera arrays placed around the operative field. These arrays transmit the information to the computer for conversion into three-dimensional (3-D) Cartesian spatial coordinates. LED systems offer the same low profile and adaptability to neurosurgical instrumentation as ultrasonic systems. However, a direct and clear line of sight is required between the localizer tool and the infrared cameras and can be difficult to achieve when patient positioning, retractors, or the operating microscope obstructs a clear line of sight. Alternatively, passive reflectors can be placed on the localizer wand or surgical instruments. Infrared signals sent from a source can reflect to the camera and convey information similar to that sent by active LED systems (Fig. 1).
Other systems have modulated magnetic fields to localize position in the operative field.[14] These systems also offer low profile wands that can be adapted to a variety of surgical instruments. Naturally, ferromagnetic surgical instruments can interfere with accuracy. In addition, the reference magnetic source, which is usually affixed to the headframe, can obstruct the full range of motion of the operating microscope. The error associated with this system is less than 4 mm. The system is subject to electronic drift and ambient electromagnetic noise.
Perhaps the most elegant solution employs the operating microscope itself as a localizer tool.[15,19] Several systems have designed operating microscopes so that their position can be tracked precisely using LED and infrared camera technology. Information about the focal length of the operating microscope and its position is tracked. All of the information is then transmitted to the computer so that the target is localized at the precise focal length of the operating microscope. In effect, the target that the neurosurgeon views through the microscope is the same target localized by the frameless stereotactic system. Many systems use two convergent laser beams to help determine when a precise focal length is reached. The laser beams must converge precisely on the structure in question at the focal length of the microscope.
Microscope-based systems must maintain the line of sight with the infrared camera. During the microsurgical portion of the procedure, they are less cumbersome than wand-based systems. Microscope-based systems, however, may be less useful than wand-based systems during the initial approach and planning of a procedure when surface landmarks or more superficial anatomy such as the location of the great sinuses may be important. For such instances, some companies have combined the option of using a hand-held localizing tool, which can be switched to the operating microscope localizer at any point during the procedure. Microscope-based systems, however, may not be as easily adaptable to specialized techniques such as stereotactic endoscopy.
Display of Data Set
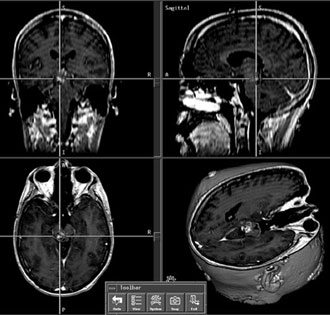
Regardless of how the data regarding target localization in space are gathered, they must be sent to a CPU. There, the information is processed with the data set previously obtained from preoperative MR or CT. The output mostly consists of a video display of the location of the probe-tip relative to the anatomical volume of the preoperative data set. Most systems offer at least four view windows: axial, coronal, and sagittal planar views correlating with the position of the localizer within that respective plane and specialized trajectory views that display along the plane of the probe itself. These views may provide useful information about the actual surgical approach to lesions. Various software adjuncts also permit 3-D constructions to window certain tissues such as skin and bone and to provide trajectory-based 3-D views of brain structures. The preoperative data set can be manipulated and areas of interest highlighted or colored so that they are visually distinct from surrounding structures. Some of the new microscope-based systems relay this video information to the microscope for a heads-up display that enables the surgeon to view both the operative field and the frameless stereotactic video output.[17]
Acquisition of Data Set
Frameless stereotaxy is adaptable to any imaging modality. Extensive work has been done with both CT and MR imaging, and each offers certain advantages. CT offers better resolution of bony structures. It appears that frameless stereotactic localization using CT is slightly more accurate than with MR imaging.[7] In contrast, MR imaging offers better visualization of soft tissue structures within the cranium and is thus the imaging modality of choice for frameless stereotaxy with most intra cranial structures.15 More recent efforts have attempted to use functional imaging such as functional magnetic resonance (fMR) imaging or spectography to incorporate functional and physiological data into the anatomical data.[15] This strategy may be particularly useful in surgery for epilepsy that involves eloquent brain tissue.[24] No doubt as neuroimaging techniques advance, they will be coupled with and incorporated into existing frameless stereotactic systems.
Anatomical Registration
All frameless stereotactic systems must be able to correlate the preoperatively acquired image data with the real-time anatomical data regarding the patient’s head position. With frame-based stereotactic systems, the patient’s brain is imaged after he or she has been placed into a headframe. As long as the patient does not shift in the headframe, the correlation between the preoperative imaging and the real-time position in space should be good. With frameless-based systems, the positional anatomical data must be “registered” against the preoperative image data set.
Most systems rely on a series of surface fiducials (Fig. 2).[2,3,7,9,11,14,15,18] Typically, the scalp is marked at least at four sites with permanent ink, and a visible and identifiable fiducial for the planned imaging modality is placed over the marks. Subsequently, the fiducial points are readily recognizable on the imaging study. Using the localizing wand to register each fiducial point allows precise correlation between preoperative imaging and operative anatomical positioning. A minimum of three fiducials is needed to triangulate accurately, but four or more are often used so that grossly inaccurate fiducial data points can be discarded.

The major disadvantage of a scalp-based fiducial system involves the relative mobility of the scalp upon the skull. Deformations of the scalp such as those produced by clamping the head in a Mayfield (Codman, Inc., Raynham, MA) headholder can shift the fiducials and thereby distort their accuracy during the registration process. However, registration accuracy tends to improve near the epicenter of the fiducials.[22] Thus, measurement inaccuracies at the surface may not necessarily reflect inaccuracies at the target.
In addition to fiducial registration systems, frameless stereotactic systems can use anatomical landmarks or surface features to register the patient’s head position.[5,8,10,11,20] Typically, such registration requires more time and data points than fiducial systems. For example, more than 40 registration points may be required when using surface registration points over the scalp. Also, the accuracy of registration based solely on anatomical landmarks such as the tragus or canthus may be less than that associated with surface fiducials.
Finally, more invasive forms of surface registration, such as the placement of a skull bolt or screw before preoperative imaging, may allow very precise registration.[20,25] These systems even obviate the need to immobilize the head during surgery because head movements relative to the frameless stereotactic system can be updated via the fixed skull screw and its triangulation with a localizing system. This procedure, however, is invasive and often requires general anesthesia.
When frameless stereotaxy is used for intracranial surgery, patient positioning proceeds as it normally would. Once imaging studies have been obtained, patients are usually brought to the OR where general endotracheal anesthesia is induced. With frameless stereotaxy, the imaging studies may be acquired without the use of monitored sedation as is required for frame-based systems. Frameless stereotactic systems can be used with patients placed in all surgical positions including supine, prone, and park-bench. The accuracy of scalp fiducials tends to be less reliable with most posterior craniotomies, likely reflecting the more mobile scalp over the posterior fossa and the posterior deformation of the scalp from lying supine on the MR imaging table. If the prone position is to be used for posterior fossa frameless stereotaxy, scalp fiducials should be placed as close as possible to the operative site. The retromastoid area offers a relatively immobile segment of the scalp for this purpose. Most intracranial procedures necessitate head immobilization with a headholder such as the Mayfield frame. Immobilization is a prerequisite for many stereotactic systems that reference themselves to the headframe. As stated, some localizing systems that use skull screws may not require head immobilization.

When the patient has been positioned and the head immobilized, the system is registered (Fig. 3). At this point, the surgeon must check the accuracy of the registration system against known anatomical landmarks such as the tragus and canthus. Minimal incisions can then be planned. The preparation and draping of the operative field must incorporate a sterile probe localizer tip and referencing system. Once a scalp flap has been created, the frameless stereotactic system can again be used to design the optimal craniotomy. Throughout the procedure, the accuracy of the wand should be assessed against known anatomical landmarks. In case accuracy deteriorates or the patient slips within the headholder, additional registration points can be identified at the beginning of the case by using anatomical landmarks such as the cranial sutures or by drilling small pits within the bone for later reregistration.
Intraoperative Imaging
Special preoperative issues must be considered with intraoperative imaging.[1] The use of imaging during the operation allows real-time update of anatomical data. This information can be used to assess the degree of tumor resection or the amount of brain shift associated with cerebrospinal fluid (CSF) drainage or tissue resection. Any intraoperative imaging system must maintain the sterile field, and these systems can be bulky and can occupy valuable OR space. Furthermore, the operating window within these devices can constrict the surgeon’s range of motion. Intraoperative MR imaging systems may require specialized instruments. Ferromagnetic tools must be avoided in the presence of a strong magnetic field. Titanium is often the metal of choice and increases the expenses for any OR that desires to use intraoperative MR imaging technology. Nonetheless, intraoperative imaging techniques represent a bridge between the goal of real-time true anatomical imaging and localization and current systems using real-time localization superimposed upon a preoperative imaging data set.
Operative Use of Frameless Stereotaxy
Frameless stereotaxy in cranial surgery is useful at all stages of an operation. The technology allows preoperative planning of the surgical approach and trajectory, enabling selection of the appropriate scalp incision, craniotomy, and corticotomy. Furthermore, important structures and anatomical landmarks may be precisely identified along the way. For example, during a supracerebellar infratentorial approach to the pineal region, all three sinuses are typically exposed to provide the greatest amount of working space. Identifying these sinuses before the craniotomy is performed minimizes the risk of injuring these structures. Frameless stereotaxy also has tremendous potential as a teaching tool for resident neurosurgeons. Frameless stereotaxy systems offer direct correlation between imaging studies and visualized anatomical structures and helps to create a 3-D conceptionalization of cerebral anatomy and a neuroradiological conceptionalization of intracranial pathology.
Frameless stereotaxy must never be a substitute for a sound understanding of intracranial anatomy. The localization error associated with most commercial systems tends to be less than 4 mm.[1,2,7-9,11,14,15] Nonetheless, inadequate registration or head movement after registration can result in localization inaccuracies, including improperly chosen approaches, extended incisions, overly large craniotomies, and inadvertent damage to neural structures. The neurosurgeon must periodically reassess the frameless stereotactic system’s accuracy against known anatomical landmarks.
Every system on the market has certain inherent inaccuracies. For example, systems relying on ultrasound depend on ambient room temperature and currents where as LED systems require a clear line of sight. The reference system used to register the data set also may be a source of error such as improper placement of fiducials or fiducial movement due to headclamp placement. Intraoperative events such as the release of large amounts of CSF, the resection of tumors, or the evacuation of blood clots can shift the location of brain structures. As a result, preoperative imaging studies may no longer represent the intraoperative anatomical reality. Techniques to minimize CSF egress by minimizing craniotomies or preserving arachnoid planes can reduce brain shift. Reregistration along internal identifiable anatomical landmarks such as the edge of the tentorium also may help minimize the effect of anatomical shifts. Finally, intraoperative MR imaging and CT techniques provide real-time updates of changes in anatomy associated with the procedure.
Although the general principles of frameless stereotaxy apply to all intra cranial surgeries, specific points and techniques for particular pathologies are addressed below. The intracranial application of frameless stereotaxy in minimally invasive procedures, functional neurosurgery, and endoscopy are addressed elsewhere in this issue.

Tumors
The marriage between frameless stereotaxy and intracranial tumor surgery is of great significance. Preoperative surgical planning, including approach and trajectory, can be defined. Tumors can be localized even if they are situated deep beneath cortical structures, and the extent of resection can be guided by frameless stereotactic imaging (Fig. 4). Frameless stereotactic guidance may be particularly important if eloquent structures abut the tumor bed. Newer imaging techniques also incorporate fMR imaging data that may prove useful in such cases.[15,24] Software enhancements associated with several frameless stereotactic systems allow the precise margins of a tumor to be outlined and colored on video display to distinguish it from surrounding structures. Much like tumors, deep-seated cerebral abscesses also benefit from frameless stereotactic localization for surgical drainage.
The most obvious tumors benefiting from frameless stereotaxy are those located deep within the brain. In these instances, even if the correct scalp incision and craniotomy are selected, localization of the lesion through the cortex can be difficult. If eloquent cortical structures are within the vicinity of the surgery, significant complications can result from errant trajectories to the tumor.
Skull base lesions also benefit from frameless stereotaxy, particularly when planning a critical approach. Skull base approaches widely remove bone structures to minimize retraction and resection of neural structures; again, frameless stereotaxy can help guide the degree of resection needed for skull base tumors. Frameless stereotaxy can also help identify prominent vascular and neural structures associated with the skull base, in effect providing a visual warning that these structures are in the vicinity during an aggressive tumor resection.
Frameless stereotaxy may prove a useful adjunct with even more readily located lesions such as convexity tumors or intraventricular tumors. With convexity or surface tumors, frameless stereotaxy can help minimize the size of the scalp incision and craniotomy, which has ramifications for cosmesis and wound healing. Although the ventricles can be cannulated using anatomical landmarks, the use of frameless stereotaxy may provide more optimal trajectories so that lesions within the ventricles can be visualized more fully.
More recently, frameless stereotaxy has been used with transsphenoidal surgery to obviate the need for intraoperative fluoroscopy.[9] In these instances, the imaging modality of choice is CT, which best images the bony structures of the nasal passages and the floor of the sphenoid sinus and sella. Although this technique offers little during the actual tumor resection, it is useful for assuring a midline trajectory through the sphenoid sinus and floor of the sella, thereby minimizing the risk to important structures such as the cavernous sinus and carotid arteries.
Some authors have also attempted to apply frameless stereotactic technique to traditional stereotactic biopsies.[5,7] In lieu of a frame, these authors have used various mechanical adjuncts to hold localization and biopsy tools rigidly along a trajectory during the biopsy. The advantage of the frameless portion of the stereotactic procedure is that multiple target points may be readily selected and optimal trajectories may be calculated “free hand.” Once they are selected, the more rigid fixation arm or device guides the bone drilling and passage of the biopsy probe. Should conversion to an open craniotomy be needed, the surgeon does not have to contend with a bulky stereotactic frame.
Figure 5. Coronal, sagittal, axial, and three-dimensional reconstruction views of a midbrain cavernous malformation. Frameless stereotaxy is essential to determine the optimal trajectory to the lesion through eloquent brain stem tissue based on the two-point method.
{kind=link}

Vascular Lesions
Just as with tumors, certain vascular lesions may be difficult to localize if they are situated within deep brain structures. Application of frameless stereotactic technique may allow precise localization as well as that of associated vascular structures feeding or draining a lesion. The two-point method applies to the localization of any intracranial lesion.[6] This technique dictates that the optimal approach to a lesion, particularly those in and around eloquent structures such as the brain stem, should be along a line connecting the lesion’s center to where it most closely abuts a pial surface.
Cavernous malformations are sometimes located deep within cerebral structures (Fig. 5). The only hint of their underlying presence may be a slight yellowish discoloration representing the deposition of hemosiderin in the surrounding cerebral tissue. Because these lesions are sometimes small and deep within cerebral structures, their precise localization is imperative. Even when it appears that a lesion reaches a pial surface on imaging studies, this may not be the case intraoperatively.[15] Frameless stereotaxy is then essential to reduce the size of the corticotomy and to minimize the morbidity associated with the resection.

The resection of arteriovenous malformations (AVMs) also benefits from frameless stereotactic technique (Fig. 6). Once important feeding and outflow vessels are identified, the AVM nidus must be removed en bloc much like a tumor. Frameless stereotaxy helps to define both the superficial and deep limits of the nidus and can help assure its complete removal. Dural AV fistulae, which often may be located by their dural attachments or their proximity to the great sinuses, can also be resected using frameless stereotaxy. Its application minimizes the scalp incision and craniotomy needed and precisely identifies large associated draining sinuses.
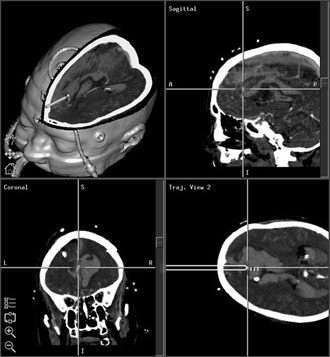
Figure 7. Three-dimensional reconstruction, sagittal, coronal, and trajectory views of an anterior communicating artery aneurysm. The significant amount of subarachnoid hemorrhage distorting the expected anatomy makes frameless stereotactic guidance useful in identifying location of the aneurysm and in defining its morphology.
{kind=link}

Frameless stereotaxy is rarely used to resect intracranial aneurysms (Fig. 7). Many of these lesions are easily localized by following the vascular tree from the circle of Willis at the skull base to the appropriate arterial branch. Frameless stereotaxy, however, may prove useful when large or complex cerebral aneurysms or associated subarachnoid hemorrhage distorts expected cerebral and vascular anatomy. If endoscopes are used to view around an aneurysm, the position of the scope tip may be localized precisely using frameless stereotactic technique.[10]

Shunts
The precise cannulation of the ventricular system and exact placement of indwelling catheter tips have been greatly facilitated by frameless ste reotaxy (Fig. 8) and may have serious implications for the efficacy and longevity of shunts. During complex fenestration procedures performed either openly or endoscopically, frameless stereotaxy may help to identify multiple cystic compartments within the ventricles that may not be readily apparent otherwise. As necessary, shunt catheters for drainage can be placed into each cystic cavity with stereotactic guidance. Long-term data regarding the efficacy of stereotactic catheter placement have yet to be collected. If the shunting procedure precludes rigid head immobilization, a skull screw or bolt can be considered to allow referencing between the preoperative imaging data set and the patient’s head position.[20]
Future Directions
Frameless stereotaxy has only been a surgical reality during the last decade. Significant advances in the technological aspects of frameless stereotactic technique are being developed rapidly. In particular, as neuroradiological modalities, including fMR imaging improve, they can be merged with existing data sets to obtain more intraoperative information. As imaging accuracy increases, the accuracy of localization will increase. Better techniques for image registration and probe tip triangulation will yield smaller margins of error. The most recent trend has been to lower the profile of the localization systems and, in some cases, to incorporate them into existing systems such as the microscope or operative tools. Video and heads-up displays within the surgical microscope will offer increasingly direct and accurate feedback to surgeons. Finally, the development of intraoperative imaging techniques will allow real-time anatomical updates to be performed to compensate for brain shifts associated with the surgical procedure. The ultimate goal of intraoperative MR imaging would be to provide real-time anatomical delineation with real-time localization.
Acknowledgment
The authors would like to thank Bradford S. Burling, Alex Islas, and Med tronic Surgical Navigation Technologies for assistance with this article.
References
- Alexander EI, Black PM, Martin C, et al: Intraoperative magnetic resonance imaging, in Alexander EI, Maciunas RJ (eds): Advanced Neurosurgical Navigation. New York: Thieme, 1999, pp 530-538
- Barnett GH, Kormos DW, Steiner CP, et al: Intraoperative localization using an armless, frameless stereotactic wand. Technical note. J Neurosurg 78:510-514, 1993a
- Barnett GH, Kormos DW, Steiner CP, et al: Use of a frameless, armless stereotactic wand for brain tumor localization with two-dimensional and three-dimensional neuroimaging. Neurosurgery 33:674-678, 1993b
- Barnett GH, Miller DW, Weisenberger J: Frameless stereotaxy with scalp-applied fiducial markers for brain biopsy procedures: Experience in 218 cases. J Neurosurg 91:569-576, 1999
- Brommeland T, Hennig R: A new procedure for frameless computer navigated stereotaxy. Acta Neurochir (Wien) 142:443-448, 2000
- Brown AP, Thompson BG, Spetzler RF: The two-point method: Evaluating brain stem lesions. BNI Quarterly 12(1):20-24, 1996
- Dorward NL, Alberti O, Palmer JD, et al: Accuracy of true frameless stereotaxy: In vivo measurement and laboratory phantom studies. Technical note. J Neurosurg 90:160-168, 1999
- Drake JM, Prudencio J, Holowka S, et al: Frameless stereotaxy in children. Pediatr Neurosurg 20:152-159, 1994
- Elias WJ, Chadduck JB, Alden TD, et al: Frameless stereotaxy for transsphenoidal surgery. Neurosurgery 45:271-277, 1999
- Frazee JG, King WA: Endoscopy and stereotaxy for aneurysms. Neurosurg Clin N Am 9:869-878, 1998
- Germano IM, Villalobos H, Silvers A, et al: Clinical use of the optical digitizer for intracranial neuro navigation. Neurosurgery 45:261-270, 1999
- Horsley V, Clarke RH: The structure and function of the cerebellum examined by a new method. Brain 31:45-124, 1908
- Iskandar BJ, Nashold BSJ: History of functional neurosurgery. Neurosurg Clin N Am 6:1-25, 1995
- Kato A, Yoshimine T, Hayakawa T, et al: A frameless, armless navigational system for computer- assisted neurosurgery. Technical note. J Neurosurg 74:845-849, 1991
- Lawton MT, Spetzler RF: Clinical experience with a frameless stereotactic arm in intracranial neurosurgery, in Alexander EI, Maciunas RJ (eds): Advanced Neurosurgical Navigation. New York: Thieme, 1999, pp 321-332
- Leksell L: A stereotactic apparatus for intracerebral surgery. Acta Chir Scand 99:229-233, 1949
- Olivier A, Germano IM, Cukiert A, et al: Frameless stereotaxy for surgery of the epilepsies: Preliminary experience. Technical note. J Neurosurg 81:629-633, 1994
- Otsubo H, Hwang PA, Hunjan A, et al: Use of frameless stereotaxy with location of electroencephalographic electrodes on three-dimensional computed tomographic images in epilepsy surgery. J Clin Neurophysiol 12:363-371, 1995
- Roberts DW, Strohbehn JW, Hatch JF, et al: A frameless stereotaxic integration of computerized tomographic imaging and the operating microscope. J Neurosurg 65:545-549, 1986
- Ryan MJ, Erickson RK, Levin DN, et al: Frameless stereotaxy with real-time tracking of patient head movement and retrospective patient-image registration. J Neurosurg 85:287-292, 1996
- Sandeman DR, Patel N, Chandler C, et al: Advances in image-directed neurosurgery: Preliminary experience with ISG Viewing Wand compared with the Leksell G frame. Br J Neurosurg 8:529-544, 1994
- Sofamor Danek: StealthStation Treatment Guidance Platform. Understanding StealthStation System Registration. Memphis: Sofamor Danek, 1999
- Spiegel EA, Wycis HT, Marks M, et al: Stereotaxic apparatus for operations on the human brain. Science 106:349-350, 1947
- Stapleton SR, Kiriakopoulos E, Mikulis D, et al: Combined utility of functional MRI, cortical mapping, and frameless stereotaxy in the resection of lesions in eloquent areas of brain in children. Pediatr Neurosurg 26:68-82, 1997
- Wang MY, Maurer CRJ, Fitzpatrick JM, et al: An automatic technique for finding and localizing externally attached markers in CT and MR volume images of the head. IEEE Trans Biomed Eng 43:627-637, 1996