


Ultrasonic Image Guidance and Resection of a Cranial Tumor: Case Report
Patrick Han, MD
Jeffrey S. Henn, MD
Bradford S. Burling, BS†
Robert F. Spetzler, MD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
†Medtronic Surgical Navigation Technologies, Louisville, CO
Abstract
Frameless stereotactic systems are being used extensively to aid in the resection of intracranial tumors. However, intraoperative shift or tumor resection can cause errors in the feedback provided by frameless stereotactic navigational systems. We present a case in which ultrasound-based technology was used to provide the surgeon information about brain shift and the extent of tumor resection to avoid such potential errors.
Key Words: frameless stereotaxy, SonoNav, ultrasound
Frameless stereotactic systems have been used extensively to aid in the resection of intracranial tumors. Typically, these systems rely on preoperative images for navigation. However, changes in anatomical relationships caused by intraoperative shifting of the intracranial contents or tumor resection can lead to significant errors in the feedback provided by frameless stereotactic systems and can cause the surgeon to abandon its use during a procedure. If the shift and resulting error go unrecognized, navigation can be inaccurate and potentially dangerous.
Intraoperative imaging can be used to recognize situations in which registration has become inaccurate and to quantitate the degree of brain shift. Options for intraoperative imaging include computed tomography (CT), magnetic resonance (MR) imaging, and ultrasonography. The following case illustrates the intraoperative use of an ultrasound-based technology[1] in the resection of a cranial meningioma.
Illustrative Case
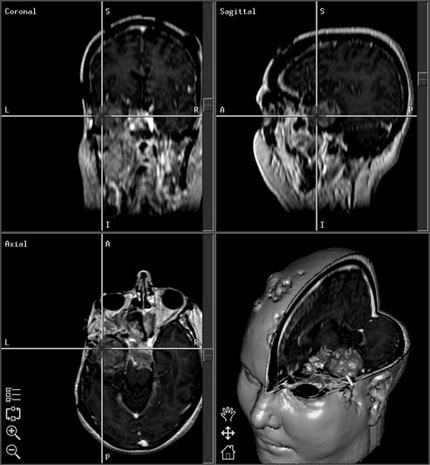
A 34-year-old female who had previously undergone resection of a left temporal malignant meningioma presented with progressive neurological decline. Upon examination, she exhibited right-sided weakness and language dysfunction. MR imaging demonstrated significant tumor recurrence involving the left temporal lobe and posterior fossa (Fig. 1). The lesion was exerting mass effect on the brain stem. The decision was made to proceed with surgical resection of the recurrent tumor.
Before surgery, the patient underwent contrast MR imaging of the brain after scalp fiducials were placed. The patient was then taken to the operating room, where anesthesia was induced. The patient was positioned in the usual fashion. A Mayfield headholder (Codman, Inc., Raynham, MA) was used for rigid fixation. At this point, the StealthStation frameless stereotactic system (Medtronic Surgical Navigation Technologies, Louis ville, CO) was registered using the standard paired-point method. After the accuracy of registration was verified, an incision and craniotomy were performed using frameless stereotactic guidance.

After the craniotomy was performed, the SonoNav system (Medtronic Surgical Navigation Technologies) was employed. This system, in conjunction with an ALOKA ultrasound unit (ALOKA, Wallingford, CT), is first incorporated into the frameless stereotactic system. The hand-held ultra sound probe includes localizing elements that allow the position of the probe to be tracked precisely in space (Fig. 2).
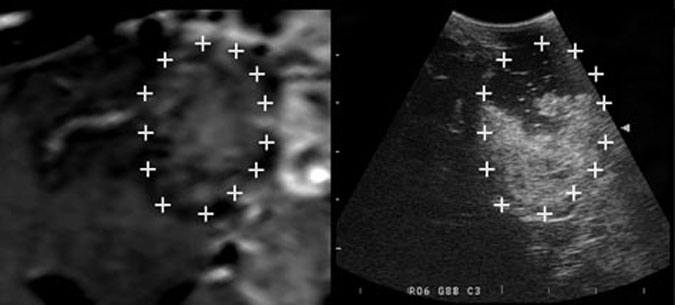
Before dural opening and throughout the resection of the tumor, the SonoNav system was used to verify the accuracy of registration and to quantitate the extent of tumor removal. There was minimal operative shift (Fig. 3).
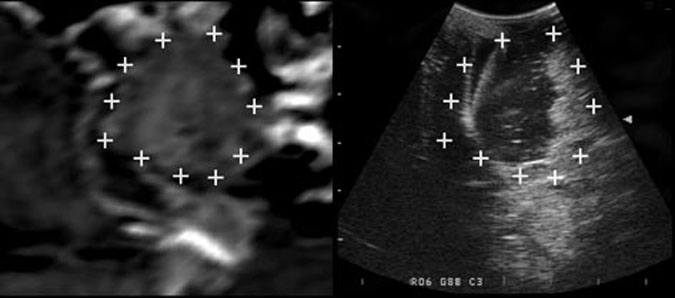
The SonoNav system was also used after the tumor was resected to rule out residual tumor (Fig. 4).
Postoperatively, the patient was discharged to home with no new deficits or complications.
Discussion
When the SonoNav probe is applied to the surface of the brain, simultaneous images, representing the planar ultrasound image and the corresponding planar view based on the preoperative imaging, are displayed. The SonoNav software also allows markers to be placed on one of the images; the corresponding points are identified on the other image. This process allows quantitative measurements of brain shift to be performed and provides a visual reference. The SonoNav unit also provides feedback about the extent of tumor resection, again, in the form of side-by-side images with the planar ultrasound im age and the preoperative image for comparison.
A major limitation of conventional frameless stereotactic systems has been that navigation is based on preoperative imaging. Changes in anatomical relationships during a procedure can lead to errors in the feedback provided by frameless stereotactic systems. The most elegant solution to this problem is the use of intraoperative MR imaging or CT to confirm the accuracy of the information provided by frameless stereotactic navigation and to determine the extent of tumor resection. Intraoperative CT and MR imaging also permit registration to be updated based on the intraoperative anatomy. Although these imaging modalities are effective, they, too, have intrinsic disadvantages. They occupy significant space and can limit the surgeon’s access to the operative field. They are also expensive and require complete restructuring of an operating room. Finally, in the case of MR imaging, the powerful magnetic field must be considered when choosing surgical instruments.
Intraoperative ultrasonography is a useful alternative for obtaining feedback about intraoperative shift and tumor resection. Although this technology does not allow registration to be updated intraoperatively, it does provide feedback when intra cranial relationships change relative to their preoperative configuration. The advantages of intraoperative ultrasonography include its low cost, ease of use, and minimal interference with the operative procedure.
This case report demonstrates how intraoperative ultrasonography can be used to provide feedback about a procedure. The ultrasound system helped to verify that intraoperative shift was minimal (Fig. 3). The system also helped delineate the degree of tumor resection. As such, Sono Nav represents a useful adjunct to frameless stereotaxy and cranial surgery.
Acknowledgment
The authors thank Medtronic Surgical Navigation Technologies for their valuable technical support.
References
- Bucholz RD, Yeh DD, Trobaugh J, et al: The correction of stereotactic inaccuracy caused by brain shift using an intraoperative ultrasound device. CRVMED-MRCAS-97 Proceedings, Grenoble, France, March 19-22, 1997, pp 459-466