


Vertex Epidural Hematoma Manifesting with Monoplegia: Case Report
Sam Safavi-Abbasi, MD
Iman Feiz-Erfan, MD
Vivek Deshmukh, MD
Christopher MacKay, MD
Shahram Partovi, MD*
Divisions of Neurological Surgery and *Neuroradiology, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
Vertex epidural hematomas are rare and usually associated with traumatic fractures of the vertex. Symptoms include headache and decreased level of consciousness, but paraplegia has also been described. The primary diagnostic modality includes a coronal computed tomographic scan of the head because these hematomas can be missed on axial slices. Surgical evacuation is the treatment of choice because even small clots can cause intracranial hypertension relative to obstruction of venous outflow. We present a patient with a traumatic vertex epidural hematoma who became symptomatic with monoplegia.
Key Words: coronal computed tomography, dural sinus obstruction, epidural hematoma, monoplegia
Epidural hematomas that occur at the vertex are a unique subtype of epidural hemorrhage and account for 1 to 8% of all extradural hematomas.[2,5,6,10] The unusual location of a vertex epidural hematoma causes an unusual clinical radiological presentation and can be a diagnostic challenge. The clinical picture of vertex epidural hematomas is variable and nonspecific, and conventional axial computed tomography (CT) can miss the clot.[6,10] The decreased use of cerebral angiography in head trauma increases the difficulty of diagnosing vertex epidural hematomas.[6,9] Consequently, diagnosis can be delayed with fatal consequences. The mortality rate is therefore high and reported to range between 18 and 50%.[8] We report the first case of a traumatic vertex epidural hematoma that became symptomatic with monoplegia.
Illustrative Case
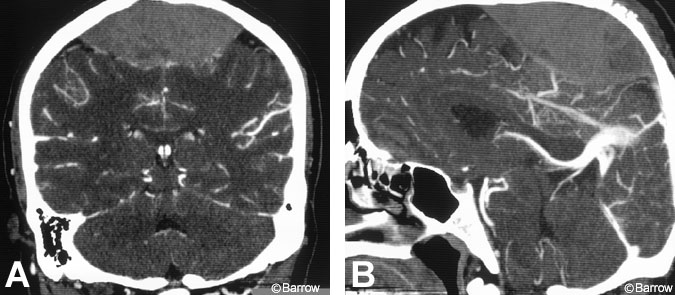
A 43-year-old Hispanic man fell down the stairs while carrying heavy machinery. He fell backward and struck the back of his head; the machinery fell across his legs. He had questionable loss of consciousness. At his initial evaluation, he was disoriented to date and place, complained about headache and bilateral lower extremity pain, and exhibited monoplegia of his left lower extremity (motor strength, 0/5) and mild weakness in his right lower extremity (motor strength, 4/5). CT of the head showed a large linear fracture crossing the vertex and an area of high density overlying both hemispheres in the highest axial cuts. Reconstruction coronal CT then clearly demonstrated a large vertex epidural hematoma (Fig.1). Radiographs of the lower extremity showed no fractures. Given his deteriorating neurological status, the patient underwent prompt surgical decompression. Generous parietal craniotomies were placed, preserving a midline keel of bone. No arterial source of bleeding was recognized, but numerous sites of brisk bleeding were present along the course of the superior sagittal sinus and parasagittal dura. Bipolar cauterization and packing were required to achieve hemostasis.
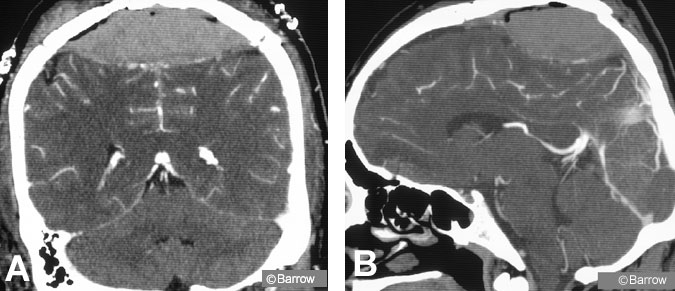

The patient’s postoperative course was marked by rapid resolution of his confusion and headache. Motor strength in his legs improved within 1 week. On postoperative Day 3, a routine follow-up CT angiogram disclosed a significant recurrence of the vertex epidural hematoma, but with patency of the superior sagittal sinus (Fig. 2). The patient was followed conservatively. No surgical intervention was performed because the patient’s clinical and neurological condition was improving. A 3-month follow-up CT scan and CT angiograms showed resolution of the recurrent hematoma and patency of the superior sagittal sinus (Fig. 3). The recurrent hematoma likely resolved through liquefaction and spontaneous drainage to the subgaleal space through the burr holes placed for the initial craniotomy. Three months after surgery, the patient had normal lower extremity sensorimotor function and normal bowel, bladder, and sexual function, with no other neurological symptoms or signs.
Discussion
Most of the reported cases of vertex epidural hematomas were caused by a traumatic injury. As many as 92 to 100% of the cases were associated with a fracture at the level of the vertex.[1,6,8,12] The associated clinical course is variable and can be acute or chronic.[6,8,10] Between 1964 and 1976, Borozone and coworkers[6] treated 14 cases of vertex epidural hematomas. Eight of these patients had an acute course, without a symptom-free interval. Stevenson and coworkers[14] reported a patient who was free of symptoms for 6 weeks but stated that most vertex epidural hematomas are acute with an urgent course. However, symptom-free intervals have varied from hours to weeks to as long as 11 months in one case.[8,10,12,14]
The clinical picture is reported to be variable and nonspecific. A review of the reported cases, however, suggests that certain signs and symptoms are recurrent. Many authors report headache, vomiting, and increased intracranial pressure (ICP) as the major clinical symptoms.[6,8,10,12] Paraplegia and motor weakness are also important manifestations.[1,6,9,11,14,16] In the series published by Borozone et al.,[2 6] of their 14 patients had hemiplegia and 5 had headache. Between 1935 and 1960, Gallagher and Browder[5] treated 167 patients with epidural hematoma and stressed the following: “One can even say that when paralysis develops on the side opposite to the cranial impact, the clinical diagnosis of extradural hematoma should preempt all others.”[2] After an extensive review of the literature, our patient appears to be the first report of a case becoming symptomatic with monoplegia. The patient’s confusing clinical picture and direct traumatic injury to his lower extremity associated with peripheral nerve irritation and pain compounded the difficulty of obtaining a diagnosis.
Alexander[1] suggested that compression of the superior sagittal sinus and subsequent compromise of the venous drainage in addition to local impairment of cerebrospinal fluid resorption are contributing factors to the increased ICP associated with a vertex epidural hematoma. Venous obstruction and direct bilateral compression of the motor strip by the clot have also been presumed to produce motor weakness and paraplegia.[1,9] Anatomically, the vertex motor cortex subserves the hips, knees, and feet, and a hematoma could directly compress these structures. Thus, mechanical compression in this area likely would produce paraplegia rather than monoplegia. The reason for this neurologic deficit in our patient remains unclear because the review of his scan revealed a centrally based clot (Fig. 1).
Alexander[1] also noted the importance of the site of venous obstruction. Anterior compromise of the superior sagittal sinus, even with a large hematoma, does not cause ICP to increase. In contrast, smaller but strategically placed posterior hematomas can cause a large increase in ICP. Consequently, even a small vertex epidural hematoma should not be underestimated.
Disruption of venous drainage was once shown by the venous phase of a carotid angiogram, which used to be the mainstay for diagnosing vertex epidural hematomas.[2,6] In addition to dilatation of cortical veins, particularly the Rolandic vein, and slowing of the circulation, Borozone and coworkers[2] reported shifting and displacement of pericallosal and callosomarginal arteries during the arterial phase. However, CT, which has become the examination of choice in patients with head trauma, may miss vertex epidural hematomas.
Many authors have noted the problems associated with the diagnosis of vertex epidural hematomas by conventional axial CT.[6,8,10,11] The difficulty arises because of the location of the clot at the apex of the brain. At this location the near-isodensity of the hematoma and bone and volume averaging effects of routine CT scanning with relatively thick slices (10 mm) make the diagnosis more difficult. Therefore, Matsumoto and coworkers[10] suggested that cerebral angiography still plays an important role and should be obtained in patients who exhibit delayed neurologic deterioration.
Most other authors emphasize coronal magnetic resonance imaging and CT as the most important diagnostic tools.[6,11,13] We believe that coronal CT scanning or coronal reconstructions are preferable and sufficient in all clinically suspected cases of vertex epidural hematomas. With coronal views, the real size of the clot can be estimated and prompt surgical intervention without a time-consuming diagnostic delay can follow. Rapid diagnosis and surgical intervention are crucial to limit complications and death from the progressive event.
Some authors believe that extradural hematomas do not always require surgical evacuation, depending on the patient’s level of consciousness and the size of the hematoma. However, this position is controversial and the exception rather than the rule.[3,4,7,15] Conservative management of vertex epidural hematomas has also been discussed.[12] Although vertex epidural hematomas have resolved spontaneously, most hematomas, especially in patients with severe symptoms of clinical deterioration, need surgical intervention. Conservative management should be chosen with great caution.
Patients can deteriorate suddenly and unpredictably. They must then undergo long-lasting, extensive, and costly neuromonitoring and serial scans. Furthermore, even small clots can become life threatening. Stevenson and coworkers[14] reported a patient who was comatose for 3 days, recovered full consciousness, was discharged, and needed surgical intervention 6 weeks after the initial trauma. This interesting case demonstrates the unpredictability of vertex epidural hematomas.
In conclusion, epidural hematoma at the vertex should be suspected in patients with skull fractures at the vertex. Patients with signs of raised ICP or paralysis, especially paresis of the lower extremity, should undergo CT scanning with thin cuts and coronal reconstructions to verify the location and size of the clot. Rapid surgical intervention, especially in patients with progressive symptoms, can limit morbidity and mortality.
References
- Alexander GL: Extradural haematoma at the vertex. J Neurol Neurosurg Psychiatry 24: 381-384, 1961
- Borozone M, Gentile S, Perria C, et al: Vertex epidural hematomas. Surg Neurol 11:277-284, 1979
- Bullock R, Smith RM, van Dellen JR: Nonoperative management of extradural hematoma. Neurosurgery 16:602-606, 1985
- Fedder SL: Management of extradural hematomas (letter). J Neurosurg 69:640, 1988
- Gallagher JP, Browder EJ: Extradural hematoma: Experience with 167 patients. J Neurosurg 29:1-12, 1968
- Guha A, Perrin RG, Grossman H, et al: Vertex epidural hematomas. Neurosurgery 25:824-828, 1998
- Hadley MN, Carter LP: Nonoperative treatment of epidural hematomas (letter). Neurosurgery 16:435, 1985
- Harbury OL, Provenzale JM, Barboriak DP: Vertex epidural hematomas: Imaging findings and diagnostic pitfalls. Eur J Radiol 36:150-157, 2000
- Liliang P-C, Liang C-L, Chen H-J, et al: Vertex epidural haematoma presented with paraplegia. Injury 32:252-253, 2001
- Matsumoto K, Akagi K, Abekura M, et al: Vertex epidural hematoma associated with traumatic arteriovenous fistula of the middle meningeal artery: A case report. Surg Neurol 55:302-304, 2001
- Messori A, Pauri F, Rychlicki F, et al: Acute posttraumatic paraplegia caused by epidural hematoma at the vertex. AJNR Am J Neuroradiol 22:1748-1749, 2001
- Miller DJ, Steinmetz M, McCutcheon IE: Vertex epidural hematoma: Surgical versus conservative management. Two case reports and review of the literature. Neurosurgery 45 :621-625, 1999
- Ramesh VG, Sivakumar S: Extradural hematoma at the vertex: A case report. Surg Neurol 43:138-139, 1995
- Stevenson GC, Brown HA, Hoyt WF: Chronic venous epidural hematoma at the vertex. J Neurosurg 21:887-891, 1964
- Tochio H, Waga S, Tashiro H, et al: Spontaneous resolution of chronic epidural hematomas: Report of three cases. Neurosurgery 15:96-100, 1984
- Wylen EL, Nanda A: Vertex epidural hematoma with coronal suture diastasis presenting with paraplegia. J Trauma 45:413-415, 1998