


Normal Pressure Hydrocephalus: Diagnostic Imaging and Prognostic Assessment
Todd R. Aho, MD
John P. Karis, MD
Division of Neuroradiology, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
Since normal pressure hydrocephalus (NPH) was first described as a clinical entity, its diagnosis has been aided by a variety of radiologic procedures and examinations. The utility of these tests for diagnosis and their ability to provide useful prognostic information pertaining to shunting have varied widely. This article reviews the radiologic modalities now used to diagnose NPH and discusses their prognostic value, with an emphasis on magnetic resonance imaging.
Key Words: computed tomography, imaging, magnetic resonance imaging, normal pressure hydrocephalus
Since first described by Adams, Fisher, and Hakim in 1965, normal pressure hydrocephalus (NPH) has mainly been diagnosed clinically.[1] Because the clinical features of NPH overlap with other types of dementia, imaging has been used to strengthen the diagnosis in uncertain cases. Different imaging modalities have also been used to help provide any potentially useful prognostic information (i.e., Will my patient benefit from shunting?). The different modalities are associated with different degrees of usefulness in the diagnosis of this disorder; some are better and some are worse than the clinical evaluation. Much research has focused on developing a useful, noninvasive prognostic test so that patients could be spared the complications associated with surgical shunting that might later prove fruitless.
There have been numerous attempts to solve this diagnostic and prognostic dilemma with various modalities, [6,7,16,24,56] and there is no consensus about which tests work and how reliable they are. For every citation touting the usefulness of a technique, another can be found in contradiction. The most recent attempts using phasecontrast magnetic resonance (MR) imaging of the cerebral aqueduct seem to hold the greatest promise. This technique, however, like all others, is not without critics. This article reviews the numerous methods still used (both the seemingly outdated and newest techniques) for diagnosis and prognosis. Imaging evaluations no longer used, such as pneumoencephalography and angiography, are not discussed.
Cisternography
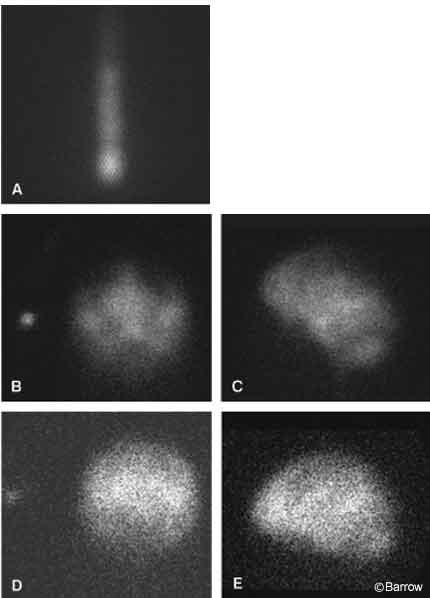
One of the first imaging modalities used in the evaluation of NPH was radionuclide cisternography. It involves injecting a radionuclide into the lumbar cerebrospinal fluid (CSF) followed by serial imaging of the brain. The major finding consistent with NPH is early ventricular reflux of the radionuclide, which persists over time (Fig. 1). The persistence of ventricular activity is the major feature that discriminates NPH from cerebral atrophy. The latter occasionally demonstrates transient reflux that does not persist beyond 24 hours (with rare exceptions). Various scoring systems have been devised based on the duration and amount of ventricular reflux as well as on the lack of radionuclide flow over the cerebral convexities, the other major finding in NPH.[5,25,29,47] Early research claimed that this examination was highly sensitive for the diagnosis of NPH and that it was also a good predictor of shunt responsiveness, particularly when using a more quantitative analysis.[37] Current research disputes this claim, finding the examination no more sensitive than clinical criteria for the diagnosis of NPH and of little prognostic value before treatment.[55] Nonetheless, the examination continues to be used, likely because it is easy to perform and familiar to referring clinicians.
Cerebral Perfusion
Cerebral perfusion has been studied extensively with nuclear medicine techniques. When compared to age-matched controls, patients with NPH tend to show decreased cerebral blood flow (CBF), another distinguishing characteristic.[31,34] Cerebral perfusion, however, is also decreased in patients with cerebral atrophy. It can be difficult, if not impossible, to distinguish the two conditions using these techniques.[36,58]
The study of cerebral perfusion may help differentiate patients with NPH from those with Alzheimer-type dementia. The latter group does not benefit from shunting. The more region-specific pattern of decreased CBF in the temporoparietal regions of patients with Alzheimer-type dementia makes this distinction possible, allows appropriate patient triage, and reduces shunt-related morbidity and mortality rates.[21]
Techniques measuring CBF also have been studied for their potential prognostic utility. Some research has shown that CBF can normalize or near normalize in certain patients after shunting.[57] In attempts to reproduce, in the short term, the physiologic situation that follows shunting, CBF has been measured in patients before and after lumbar puncture. Some studies have found this technique to be highly useful, while others have been unable to reproduce these results.[34,36,42,58]
The major difficulty with analyzing the data concerning these techniques is the lack of standardization. Some studies have used planar imaging, and others have used cross-sectional imaging with single photon emission computed tomography (SPECT) or positron emission tomography (PET). Radiotracers and their routes of administration have varied. The time elapsed before re-imaging on postlumbar puncture studies has also varied among studies, making direct comparison of data difficult. Furthermore, the analysis of such studies is complex and these modalities are not widely available.
Cerebral Metabolism
Studies of the brain with[18] F-fluorodeoxyglucose (FDG)-PET have demonstrated globally decreased brain metabolism in patients with NPH compared with controls. The major utility of this examination is the possible diagnosis of Alzheimer-type dementia in patients with ambiguous clinical findings. The regional pattern of hypometabolism, mostly affecting the temporoparietal lobes, allows this disorder to be differentiated from other causes of dementia, including NPH.[21,28]
Transcranial Doppler Ultrasonography
Historically, the use of ultrasonography in the evaluation of NPH has been limited because ultrasound penetrates the calvarium poorly. New advances, specifically transcranial Doppler (TCD) ultrasonography, allow more in-depth analysis of this technique in the adult brain. With this technique, cerebrovascular CO2 reactivity also can be measured to obtain a measure of the vasodilatory capacity of the brain.
This technique has been used to study cerebral hemodynamics in NPH, both pre- and postoperatively. In one study that used preoperative imaging, patients with normal or near normal CO2 reactivity before surgery showed the greatest clinical improvement after treatment.[17] Other studies that included both pre- and postoperative imaging have demonstrated that postoperative patients who responded positively to shunting had statistically significant increases in CO2 reactivity in the anterior cerebral arteries, middle cerebral arteries, or both after surgery.[2,39]
From a diagnostic perspective, patients with impaired autoregulation (i.e., CO2 reactivity) demonstrate increased resistance to CSF outflow on combined studies. The latter is associated with atrophy. In comparison, NPH patients most often exhibit increased resistance to CSF outflow while autoregulation tends to be preserved.[10]
Measurements of the velocity of CBF with this technique have varied. Studies have shown both unchanged and decreased velocities after shunting.[2,39] In the latter instance, patients with the highest preoperative end diastolic velocities and mean flow velocities were found to derive the greatest benefit from shunting.[2] This technique has also been used in conjunction with continuous intracranial pressure (ICP) monitoring to improve understanding of the physiologic basis of B waves, the cornerstone of ICP monitoring commonly used to triage patients.[12,13]
In general, TCD has not been used to diagnose or to plan treatment of NPH. It is performed at few institutions, especially in the United States. However, observations obtained with this technique may improve our understanding of the pathophysiology of this disorder and eventually may provide useful prognostic information.
Computed Tomography
The advent of computed tomography (CT), with its much improved visualization of the brain and ventricular system compared with earlier studies, was a huge advance in the evaluation of most diseases of the central nervous system, not the least of which was NPH. Hydrocephalus, the cornerstone of the diagnosis, could be well evaluated in a quick, noninvasive manner. CT easily shows the presence and extent of hydrocephalus as well as the degree of existing cortical atrophy. The latter was poorly evaluated with earlier imaging modalities such as pneumoencephalography and cisternography.
The CT diagnosis of NPH relied on certain observations: enlargement of the lateral and third ventricles, enlargement of the temporal horns, prominent basilar cisterns, enlarged suprasellar cistern, nonvisualization of the high cerebral convexity sulci, and possible enlargement of the fourth ventricle.[38,50] Research has focused on the degree of temporal horn dilatation, which is thought to be more specific to the diagnosis of NPH than atrophy. Temporal horn enlargement on CT strongly correlates with positive findings on radionuclide cisternography.[38] The Evans’ or frontal horn ratio is the parameter most commonly studied and documented. It consists of the measured distance of the frontal horns divided by the width of the inner table of the calvarium at the same level. Ratios greater than 0.32 are consistent with the diagnosis of NPH.[24,56] There is some overlap in Evans’ ratio between patients with NPH and those with atrophy, and this parameter does not discriminate between NPH and obstructive hydrocephalus. Research into potential prognostic information obtained from the degree or distribution of hydrocephalus has identified no single significant finding to correlate with postoperative improvement.[22,27,59] Over time, increasing overlap in the presence of sulcal prominence between NPH and atrophy patients was further documented, with the acknowledgment that some degree of atrophy is common in NPH patients.[38] However, the degree of ventricular prominence is still disproportionate to sulcal prominence, a finding heavily used today to interpret CT findings.
CT also allows assessment of the degree of associated white matter changes in the periventricular regions. Originally, these changes were described as a negative prognostic factor for the response of patients to shunting. Most of the current data on this subject concern the MR imaging evaluation of these abnormalities and are discussed below in the section devoted to that modality.
CT Cisternography
Cisternography, as originally described with radionuclides, has also been performed with iodinated contrast. Studies evaluating both techniques have verified that CSF kinetics are similar with both techniques. Possible advantages of the CT technique include direct visualization of intrathecal injection under fluoroscopy (i.e., decreasing the number of failed examinations caused by inaccurate needle positioning) and improved spatial resolution, possibly for quantitative analysis. In its original form, however, this examination poorly evaluated flow at the cerebral convexities, which is more easily seen with the radionuclide technique. CT was also more susceptible to motion artifact, which is common with demented patients. Overall, no great advantage of CT cisternography over the radionuclide technique has been demonstrated.[15]
CT Perfusion
CBF has been studied using different CT methods such as dynamic iodinated contrast enhancement and the xenon-inhalation method. Results have mirrored and are concordant with those of nuclear medicine perfusion: globally decreased CBF (± regional variations) with improvements identified after shunting (in responding patients).[41,51] These studies have yielded no useful prognostic information.
MR Imaging
The initial assessment of NPH using MR imaging involved some of the parameters introduced with CT, that is, evaluation of the ventricular system and assessment of coexisting cortical atrophy.[18] The presence or absence of associated white matter changes, particularly within the periventricular white matter, became the subject of intense investigation because MR imaging much improved their visualization. The effect of these white matter changes on clinical improvement after shunting has been a question of particular interest.
Initial research demonstrated that these white matter changes were associated with negative outcomes after shunting, to the point that their presence was deemed a contraindication to surgery.[52] More recent research has determined that this stance is inappropriate. Patients with even severe white matter changes on MR imaging can benefit from surgical shunting and can indeed have excellent clinical outcomes. The presence of these changes, however, is still considered a negative prognostic indicator.[20,32,54]
These white matter changes have also been implicated in the pathogenesis of NPH, but whether the relationship is cause or effect is debated. Some authors believe the changes may represent deep white matter infarcts, which lead to a reduction in periventricular tensile strength and initiate the development of NPH. Others argue that these changes follow transependymal CSF diffusion from the hydrocephalus itself.[6,32,54]
The overall “health” of the periventricular white matter has been studied in NPH patients using an MR imaging technique called magnetization transfer (MT). This technique measures the interaction between the pool of unbound water protons in tissue and the pool of water protons bound to macromolecules such as proteins and membranes. Healthy white matter (in normal volunteers) has a significantly higher rate of MT than even normal-appearing white matter in NPH patients. This finding indicates that white matter damage exists before it can be detected by routine imaging.[23] The cause of this damage, however, is still uncertain. This technique eventually may prove to have prognostic implications, based on the negative correlation between the extent of white matter disease and degree of postoperative improvement.
Three-dimensional (3D) MR imaging techniques can be used to improve the diagnosis of NPH. Using 3D MR imaging, Tsunoda et al. compared the total intracranial and ventricular CSF volumes in patients with NPH to those of normal, age-matched controls and patients with cerebrovascular disease.[53] Patients with cerebrovascular disease had the largest total intracranial CSF volumes. However, patients with NPH had ventricular volume-to-total intracranial volume ratios that were significantly higher than those of both comparison groups. In fact, these ratios were greater than 30% only in patients with NPH, allowing their differentiation with a high degree of specificity. Three-dimensional MR imaging has also been used to differentiate patients with NPH from patients with Alzheimer’s disease by evaluating hippocampal volumes and the size of perihippocampal fissures.[26,49] Patients with Alzheimer’s disease have significantly decreased hippocampal volumes compared to both NPH patients and normal age-matched controls.[49] Subjective and objective analyses of the size of perihippocampal fissures between the two groups yielded statistically significant larger sizes in the group with Alzheimer’s disease. The subjective analysis was almost as robust as the objective analysis.[26]
MR has also been used to study the pathophysiology of NPH by evaluating the presence of decreased vascular compliance in the superior sagittal sinus and straight sinus in NPH patients. Bateman[3,4] demonstrated that vascular compliance in NPH patients was decreased compared to control patients with and without cerebral atrophy. Interestingly, vascular compliance in NPH patients studied after CSF was removed approximated values seen in the control groups, possibly giving further insight into the pathophysiology of this disorder.
CSF Flow
The use of MR imaging to evaluate the dynamics of CSF flow was first qualitative. Quantitative measurement of flow velocity and the flow volume through the cerebral aqueduct then followed.
Early in the use of MR imaging a signal void was often seen in the cerebral aqueduct. Furthermore, the signal void observed in patients with hydrocephalus was often more pronounced than that seen in patients with normal ventricles. The most common explanation for these findings was the presence of higher volume, turbulent CSF flow in these patients. This finding was later used in attempts to triage patients to CSF shunting based on the appearance and extent of the flow void.[9,33,35,43]
In 1991 Bradley et al. suggested that patients with an increased flow void on MR imaging were more likely to have a good or excellent response to shunting.[9] In 1993 Mascalchi et al. prospectively demonstrated the possible utility of this finding in predicting shunt-responsiveness using a qualitative, gradient-echo ciné technique.[43] Other research, including a study by Krauss et al. in 1997, disputed this finding. The degree and extension of the CSF flow void were thought to provide little predictive value for the outcome of shunting.[33]
Assessment of this sign is plagued by features seen with the assessment of other possibly useful measures of NPH, mostly nonuniformity of parameters. Information gleaned from the original research may be unavailable or may not be comparable because of these changes. These possibilities render correspondences and discrepancies between these research studies less valid.[6]
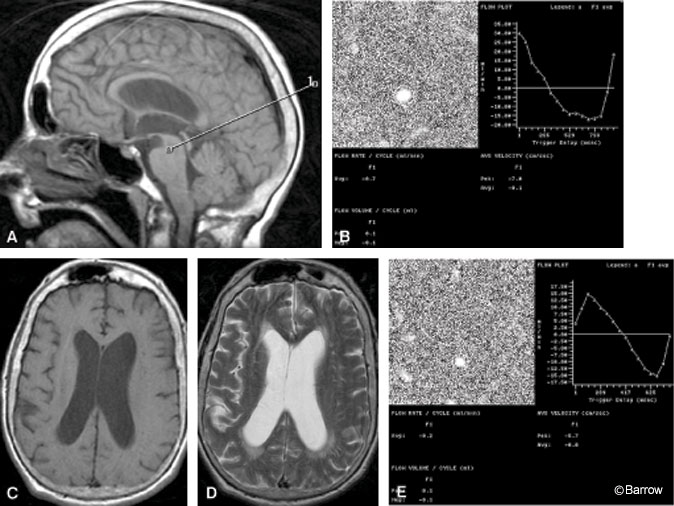
The most recent study to garner interest is phase-contrast MR imaging. This velocity-sensitive technique allows both the velocity and volume of CSF to be determined (Fig. 2). The technique has been used to study obstructive and nonobstructive hydrocephalus, with evaluation of the cerebral aqueduct of greatest concern.[45] Strong correlation between these studies and other invasive studies, such as continuous ICP monitoring, supports the validity of the technique.[48]
Early phase-contrast MR imaging flow studies measured CSF velocity through the aqueduct. Flow velocities in patients with NPH were elevated compared to those in normal controls. Occasionally, however, aqueductal flow velocities overlapped between NPH and nonNPH patients.[44] Further investigation into the value of flow volume, which also accounts for aqueductal size, began.
In 1994 Gideon et al. were among the first to document elevated CSF flow volumes through the aqueduct in NPH patients when compared with healthy volunteers. This work demonstrated the usefulness of this technique for diagnosis.[19] Luetmer et al. suggested a cut-off point at which the diagnosis of NPH can be made with a high degree of certainty (18 ml/min).[40]
The prognostic value of phase-contrast MR imaging has also been evaluated.[8,11,14,30,46] Bradley et al. found that 12 of 12 patients with aqueductal stroke volumes greater than 42 mcL/cycle showed a favorable response to shunting. The correlation was statistically significant. However, three of all patients with lower stroke volumes also benefited from shunting.[8]
All studies evaluating the prognostic value of this technique agree on one principle: Patients with very elevated stroke volumes are likely to have a positive response to shunting. Disagreements arise about where to place the cut-off point—the “gray-zone” where responders and nonresponders overlap. In a small study by Parkkola et al., patients with flow volumes at or above 10 mL/min demonstrated positive responses to shunting.[46] In a large study by Dixon et al., all patients with stroke volumes greater than 33 mL/min improved after shunting.[11] However, there was no significant association between mean CSF flow and degree of improvement. Nor was there an apparent threshold value for CSF flow below which patients did not improve. Further evaluation of this technique, especially involving prospective analysis, is warranted.
Conclusions
Multiple imaging modalities have been studied in the evaluation of NPH. Many of these modalities have enabled NPH to be diagnosed with considerable certainty. Some studies have provided potentially useful data concerning the possible pathophysiology of this disorder, and the utility of some studies for prognosis after shunting remains controversial. A variety of different imaging techniques continues to be used on a routine basis, either because they are familiar to clinicians or because opinions about the validity of the research differ.
At our institution the team of physicians addressing this disorder has focused its efforts on the MR imaging measurement of aqueductal stroke volume. This technique is thought to give direct information about decreased brain elasticity and compliance (a current theory of NPH pathophysiology) and is minimally affected by variations in heart rate. It is hoped that further prospective analysis of this technique will help to define its role in the diagnosis and preoperative prognosis of patients with NPH.
References
- Adams RD, Fisher CM, Hakim S, et al: Symptomatic occult hydrocephalus with “normal” cerebrospinal fluid pressure. A treatable syndrome. N Engl J Med 273:117-126, 1965
- Bakker SL, Boon AJ, Wijnhoud AD, et al: Cerebral hemodynamics before and after shunting in normal pressure hydrocephalus. Acta Neurol Scand 106:123-127, 2002
- Bateman GA: Vascular compliance in normal pressure hydrocephalus. AJNR Am J Neuroradiol 21:1574-1585, 2000
- Bateman GA: Toward a better understanding of normal pressure hydrocephalus. AJNR Am J Neuroradiol 22:596, 2001
- Benson DF, LeMay M, Patten DH, et al: Diagnosis of normal-pressure hydrocephalus. N Engl J Med 283:609-615, 1970
- Bradley WG: Normal pressure hydrocephalus: New concepts on etiology and diagnosis. AJNR Am J Neuroradiol 21:1586-1590, 2000
- Bradley WG, Jr.: Diagnostic tools in hydrocephalus. Neurosurg Clin N Am 12:661-684, 2001
- Bradley WG, Jr., Scalzo D, Queralt J, et al: Normal-
pressure hydrocephalus: Evaluation with cerebrospinal fluid flow measurements at MR imaging. Radiology 198:523-529, 1996 - Bradley WG, Jr., Whittemore AR, Kortman KE, et al: Marked cerebrospinal fluid void: Indicator of successful shunt in patients with suspected normal-pressure hydrocephalus. Radiology 178:459-466, 1991
- Czosnyka ZH, Czosnyka M, Whitfield PC, et al: Cerebral autoregulation among patients with symptoms of hydrocephalus. Neurosurgery 50:526-533, 2002
- Dixon GR, Friedman JA, Luetmer PH, et al: Use of cerebrospinal fluid flow rates measured by phase-contrast MR to predict outcome of ventriculoperitoneal shunting for idiopathic normalpressure hydrocephalus. Mayo Clin Proc 77:509-514, 2002
- Droste DW, Krauss JK: Simultaneous recording of cerebrospinal fluid pressure and middle cerebral artery blood flow velocity in patients with suspected symptomatic normal pressure hydrocephalus. J Neurol Neurosurg Psychiatry 56:75-79, 1993
- Droste DW, Krauss JK, Berger W, et al: Rhythmic oscillations with a wavelength of 0.5-2 min in transcranial Doppler recordings. Acta Neurol Scand 90:99-104, 1994
- Egeler-Peerdeman SM, Barkhof F, Walchenbach R, et al: Cine phase-contrast MR imaging in normal pressure hydrocephalus patients: relation to surgical outcome. Acta Neurochir Suppl (Wien) 71:340-342, 1998
- Enzmann DR, Norman D, Price DC, et al: Metrizamide and radionuclide cisternography in communicating hydrocephalus. Radiology 130:681-686, 1979
- Fishman RA, Dillon WP: Normal pressure hydrocephalus: New findings and old questions. AJNR Am J Neuroradiol 22:1640-1641, 2001
- Fritz W, Kalbarczyk H, Schmidt K: Transcranial Doppler sonographic identification of a subgroup of patients with normal pressure hydrocephalus with coexistent vascular disease and treatment failure. Neurosurgery 25:777-780, 1989
- Gammal TE, Allen MB, Jr., Brooks BS, et al: MR evaluation of hydrocephalus. AJR Am J Roentgenol 149:807-813, 1987
- Gideon P, Stahlberg F, Thomsen C, et al: Cerebrospinal fluid flow and production in patients with normal pressure hydrocephalus studied by MRI. Neuroradiology 36:210-215, 1994
- Godersky JC, Graff-Radford NR, Yuh WT: Magnetic resonance imaging of patients with normal pressure hydrocephalus. Adv Neurol 52:554, 1990
- Granado JM, Diaz F, Alday R: Evaluation of brain SPECT in the diagnosis and prognosis of the normal pressure hydrocephalus syndrome. Acta Neurochir (Wien) 112:88-91, 1991
- Gunasekera L, Richardson AE: Computerized axial tomography in idiopathic hydrocephalus. Brain 100:749-754, 1977
- Hahnel S, Freund M, Munkel K, et al: Magnetisation transfer ratio is low in normal-appearing cerebral white matter in patients with normal pressure hydrocephalus. Neuroradiology 42:174-179, 2000
- Hebb AO, Cusimano MD: Idiopathic normal pressure hydrocephalus: A systematic review of diagnosis and outcome. Neurosurgery 49: 1166-1186, 2001
- Heinz ER, Davis DO, Karp HR: Abnormal isotope cisternography in symptomatic (sic) occult hydrocephalus. A correlative isotopic-neuroradiological study in 130 subjects. Radiology 95:109-120, 1970
- Holodny AI, Waxman R, George AE, et al: MR differential diagnosis of normal-pressure hydrocephalus and Alzheimer disease: Significance of perihippocampal fissures. AJNR Am J Neuroradiol 19:813-819, 1998
- Jacobs L, Kinkel W: Computerized axial transverse tomography in normal pressure hydrocephalus. Neurology 26:501-507, 1976
- Jagust WJ, Friedland RP, Budinger TF: Positron emission tomography with [18F] fluorodeoxyglucose differentiates normal pressure hydrocephalus from Alzheimer-type dementia. J Neurol Neurosurg Psychiatry 48:1091-1096, 1985
- James AE, Jr., DeLand FH, Hodges FJ 3rd, et al: Normal-pressure hydrocephalus. Role of cisternography in diagnosis. JAMA 213:1615-1622, 1970
- Kim DS, Choi JU, Huh R, et al: Quantitative assessment of cerebrospinal fluid hydrodynamics using a phase-contrast cine MR image in hydrocephalus. Childs Nerv Syst 15:461-467, 1999
- Klinge-Xhemajli P, Heissler HE, Fischer J, et al: Cerebral blood flow in chronic hydrocephalus—a parameter indicating shunt failure—new aspects. Acta Neurochir Suppl (Wien) 71:347-349, 1998
- Krauss JK, Droste DW, Vach W, et al: Cerebrospinal fluid shunting in idiopathic normalpressure hydrocephalus of the elderly: Effect of periventricular and deep white matter lesions. Neurosurgery 39:292-300, 1996
- Krauss JK, Regel JP, Vach W, et al: Flow void of cerebrospinal fluid in idiopathic normal pressure hydrocephalus of the elderly: Can it predict outcome after shunting? Neurosurgery 40:67-74, 1997
- Kristensen B, Malm J, Fagerland M, et al: Regional cerebral blood flow, white matter abnormalities, and cerebrospinal fluid hydrodynamics in patients with idiopathic adult hydrocephalus syndrome. J Neurol Neurosurg Psychiatry 60:282-288, 1996
- Kunz U, Heintz P, Ehrenheim C, et al: MRI as the primary diagnostic instrument in normal pressure hydrocephalus? Psychiatry Res 29:287-288, 1989
- Kushner M, Younkin D, Weinberger J, et al: Cerebral hemodynamics in the diagnosis of normal pressure hydrocephalus. Neurology 34:96-99, 1984
- Larsson A, Moonen M, Bergh AC, et al: Predictive value of quantitative cisternography in normal pressure hydrocephalus. Acta Neurol Scand 81:327-332, 1990
- Leborgne JM, Sheldon JJ, Goldstein MS, et al: Differential diagnosis between pressure hydrocephalus and cerebral atrophy on computed tomography. Rev Interam Radiol 4:75-78, 1979
- Lee EJ, Hung YC, Chang CH, et al: Cerebral blood flow velocity and vasomotor reactivity before and after shunting surgery in patients with normal pressure hydrocephalus. Acta Neurochir (Wien) 140:599-605, 1998
- Luetmer PH, Huston J, Friedman JA, et al: Measurement of cerebrospinal fluid flow at the cerebral aqueduct by use of phase-contrast magnetic resonance imaging: Technique validation and utility in diagnosing idiopathic normal pressure hydrocephalus. Neurosurgery 50:534-544, 2002
- Maeder P, de Tribolet N: Xenon CT measurement of cerebral blood flow in hydrocephalus. Childs Nerv Syst 11:388-391, 1995
- Mamo HL, Meric PC, Ponsin JC, et al: Cerebral blood flow in normal pressure hydrocephalus. Stroke 18:1074-1080, 1987
- Mascalchi M, Arnetoli G, Inzitari D, et al: Cine-MR imaging of aqueductal CSF flow in normal pressure hydrocephalus syndrome before and after CSF shunt. Acta Radiol 34:586-592, 1993
- Mase M, Yamada K, Banno T, et al: Quantitative analysis of CSF flow dynamics using MRI in normal pressure hydrocephalus. Acta Neurochir Suppl (Wien) 71:350-353, 1998
- Nitz WR, Bradley WG, Jr., Watanabe AS, et al: Flow dynamics of cerebrospinal fluid: Assessment with phase-contrast velocity MR imaging performed with retrospective cardiac gating. Radiology 183:395-405, 1992
- Parkkola RK, Komu ME, Kotilainen EM, et al: Cerebrospinal fluid flow in patients with dilated ventricles studied with MR imaging. Eur Radiol 10:1442-1446, 2000
- Patten DH, Benson DF: Diagnosis of normalpressure hydrocephalus by RISA cisternography. J Nucl Med 9:457-461, 1968
- Poca MA, Sahuquillo J, Busto M, et al: Agreement between CSF flow dynamics in MRI and ICP monitoring in the diagnosis of normal pressure hydrocephalus. Sensitivity and specificity of CSF dynamics to predict outcome. Acta Neurochir Suppl 81:7-10, 2002
- Savolainen S, Laakso MP, Paljarvi L, et al: MR imaging of the hippocampus in normal pressure hydrocephalus: Correlations with cortical Alzheimer’s disease confirmed by pathologic analysis. AJNR Am J Neuroradiol 21:409-414, 2000
- Soo YS, Hatfield KD, Segal SD: The value and limitations of computerized axial tomography (CT) in the management of normal pressure hydrocephalus (NPH). Australas Radiol 23:96-104, 1979
- Tamaki N, Kusunoki T, Wakabayashi T, et al: Cerebral hemodynamics in normal-pressure hydrocephalus. Evaluation by 133Xe inhalation method and dynamic CT study. J Neurosurg 61:510-514, 1984
- Tans JT, Boon AJ, Dutch NPH Study Group: How to select patients with normal pressure hydrocephalus for shunting. Acta Neurochir Suppl 81:3-5, 2002
- Tsunoda A, Mitsuoka H, Sato K, et al: A quantitative index of intracranial cerebrospinal fluid distribution in normal pressure hydrocephalus using an MRI-based processing technique. Neuroradiology 42:424-429, 2000
- Tullberg M, Jensen C, Ekholm S, et al: Normal pressure hydrocephalus: Vascular white matter changes on MR images must not exclude patients from shunt surgery. AJNR Am J Neuroradiol 22:1665-1673, 2001
- Vanneste J, Augustijn P, Davies GA, et al: Normal-pressure hydrocephalus. Is cisternography still useful in selecting patients for a shunt? Arch Neurol 49:366-370, 1992
- Vanneste JA: Diagnosis and management of normal-pressure hydrocephalus. J Neurol 247: 5-14, 2003
- Vorstrup S, Christensen J, Gjerris F, et al: Cerebral blood flow in patients with normal-pressure hydrocephalus before and after shunting. J Neurosurg 66:379-387, 1987
- Waldemar G, Schmidt JF, Delecluse F, et al: High resolution SPECT with [99mTc]-d,1-HMPAO in normal pressure hydrocephalus before and after shunt operation. J Neurol Neurosurg Psychiatry 56:655-664, 1993
- Wikkelso C, Andersson H, Blomstrand C, et al: Computed tomography of the brain in the diagnosis of the prognosis in normal pressure hydrocephalus. Neuroradiology 31:160-165, 1989