


Surgical Management of Hypothalamic Hamartomas
Iman Feiz-Erfan, MD
Harold L. Rekate, MD
Andrew G. Shetter, MD
Rungsak Siwanuwatn, MD*
Eric M. Horn, MD, PhD
Robert F. Spetzler, MD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
*Current Address: Division of Neurological Surgery, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Abstract
Hypothalamic hamartomas are rare developmental abnormalities known to cause various types of seizures, behavioral disturbances, rage attacks, and precocious puberty. Gelastic (laughing) seizures, the most characteristic type, are refractory to medical management. If uncontrolled, the seizures can lead to progressive cognitive and behavioral decline. Surgery may be effective in managing the seizures associated with hypothalamic hamartomas. The introduction of the transcallosal anterior interforniceal approach has improved the resectability of these lesions and is associated with a higher likelihood of seizure control compared to the more traditional frontotemporal pterional, transsylvian, and subtemporal approaches. Skull base approaches through an orbitozygomatic osteotomy are other surgical options for resecting these lesions. This article reviews the surgical management of hypothalamic hamartomas at the Barrow Neurological Institute.
Key Words: hamartoma, hypothalamus, seizures, surgical approach
Hypothalamic hamartomas cause a variety of symptoms. They may be associated with precocious puberty, gelastic seizures, mental retardation, and behavioral disturbances, particularly aggressive behavior and visual impairment.[4,5,11,21,28,33,34] Clinico-anatomically, these lesions have been divided into two main subsets. One group, called pedunculated hamartomas or parahypothalamic hamartomas, often has a narrower base attached to the floor of the hypothalamus and appears not to arise within the hypothalamus. These lesions seem more likely to be associated with precocious puberty and less often with gelastic seizures. The second subset, sessile or intrahypothalamic hamartomas, has a broad attachment to the hypothalamus. They appear to lie within the substance of the hypothalamus itself and may distort the contour of the third ventricle. These hamartomas most often seem to be associated with gelastic seizures and less frequently with precocious puberty.[4,6,8,13,33]
Indications for Surgery
Before the advent of medical therapy for precocious puberty, hypothalamic hamartomas causing this condition were resected surgically to cure the endocrinological abnormality.[25] Surgical resection is still necessary if medical therapy fails to improve precocious puberty or if a neurological deficit is caused by the mass effect of the hamartoma.[20,21] No effective medical therapy is available to control the gelastic seizures associated with hamartomas. [5,31] Seizures tend to appear right after birth and worsen progressively, with the secondary development of complex partial seizures, drop attacks, tonic seizures, tonic-clonic seizures, and secondary generalized seizures.[5,22,31,33] Some patients tend to show significant progressive cognitive and functional decline over time if their seizures remain poorly controlled.[5] Many of these patients often show evidence of mental retardation and aggressive behavior.[5]
Surgical treatment has consisted of focal corticectomy, corpus callosotomy, or resection of the hypothalamic hamartoma. Focal corticectomy has primarily been performed after electroencephalographic (EEG) monitoring has identified an epileptic focus in a distinct lobe. Neither a focal corticectomy nor a corpus callosotomy controls the gelastic seizures of patients with hypothalamic hamartomas.[7] In terms of controlling gelastic seizures, the best surgical outcomes have been obtained by direct resection of the hamartoma. The overall success rate for curing or reducing seizures after resection of hypothalamic hamartomas causing gelastic seizures is about 52%.[17]
The primary surgical approach that has been used to resect hypothalamic hamartomas is the subfrontal-subtemporal approach. Numerous modifications of this approach, including entering the third ventricle via the lamina terminalis, have been described.[17]
The efficacy of surgical treatment of gelastic seizures associated with hypothalamic hamartoma increased after the transcallosal anterior interforniceal approach was introduced.[28] The introduction of skull base approaches improved visualization of hypothalamic hamartomas from below, thereby facilitating their resection, especially the pedunculated subtype.[10,15,21,29] After these procedures, the behavioral and cognitive deficits of several patients have improved significantly.
The Barrow Experience
Before 2003, four patients with intractable epilepsy caused by hypothalamic hamartoma underwent surgical treatment at Barrow. Surgical procedures included the orbitozygomatic approach in three patients and an endoscopic removal in one patient. After undergoing an orbitozygomatic approach, two patients were free of seizures as was the patient who underwent endoscopic resection. After an orbitozygomatic approach and debulking of the hamartoma, the frequency of one patient’s seizures decreased. Except for the endoscopic procedure, the resections began at the lowest bulge of the hamartoma and worked toward the normal hypothalamus. During these cases, it was difficult to determine the extent of resection as the operations proceeded.
Confronting the same concerns, Professor Jeffrey Rosenfeld and colleagues from Melbourne, Australia[28] believed that more complete resection of these masses could be achieved by approaching them from above. He researched the issue and performed anatomic studies to determine the best approach to these lesions. Based on his investigations, he used the transcallosal anterior interforniceal approach to the third ventricle to resect hypothalamic hamartomas successfully in five patients.
As a result of his experience, patients from all over the world flew to Melbourne for surgical treatment. Professor Rosenfeld recognized that it was difficult for patients to travel to and from Australia and decided to teach his techniques to neurosurgical centers on other continents. He selected Barrow, a center in Oxford in the United Kingdom, and a center in Singapore to perform the procedures. In February 2003, he traveled to the United States as a visiting professor at Barrow. During that time, he worked with Drs. Rekate and Spetzler to perform transcallosal interforniceal surgery on six patients with intractable epilepsy and hypothalamic hamartoma. Since then and with the help of the Hypothalamic Hamartoma Support Group (https://www.hhugs.com/), Barrow has developed a comprehensive program for the assessment and treatment of patients with hypothalamic hamartomas as described elsewhere in this issue.
Surgical Options for Treating Hypothalamic Hamartomas
The following options are available for the surgical management of hypothalamic hamartomas. Each has its own indications, depending on size and anatomical location of a given hypothalamic hamartoma and the goals of the surgical procedure.
Pterional Approach With or Without Removal of the Supraorbital Bar
For very rare lesions such as hypothalamic hamartomas, a specific approach cannot be identified as the traditional approach. However, most surgery for hypothalamic hamartomas has involved splitting the sylvian fissure and approaching the mass between the ipsilateral carotid artery and optic and oculomotor nerves with or without opening the lamina terminalis to access the third ventricle. This approach is the most direct route to lesions in this location, and the mass can be entered without traversing normal tissue. The approach is ideal for the purely pedunculated hamartomas associated with precocious puberty.[2,18,30]
However, large masses within the third ventricle with an extensive attachment to the lateral walls of the third ventricle or hypothalamus cannot be fully removed or disconnected using this approach. As the surgeon removes the mass, the surgical instruments are moved toward the vital structures of the hypothalamus. It is difficult to know when resection should stop even though a difference in color and texture between the hamartoma and the normal brain structures can be observed. Hamartomas tend to be gray in contrast to the white of normal brain tissue. The texture of the lesions is also somewhat softer than normal brain tissue. The corridors for removing the mass in this location are limited even after the lamina terminalis is opened. Complete resection must be performed around a corner from the optic apparatus, and near the end of the operation the procedure is performed blindly. Despite incomplete removal of the mass, patients can be freed from seizures as long as the hamartoma is disconnected from the bordering hypothalamus.[28] This part of the surgery is the most difficult to accomplish through a pterional or extended orbitozygomatic pterional approach.
Illustrative Case 1
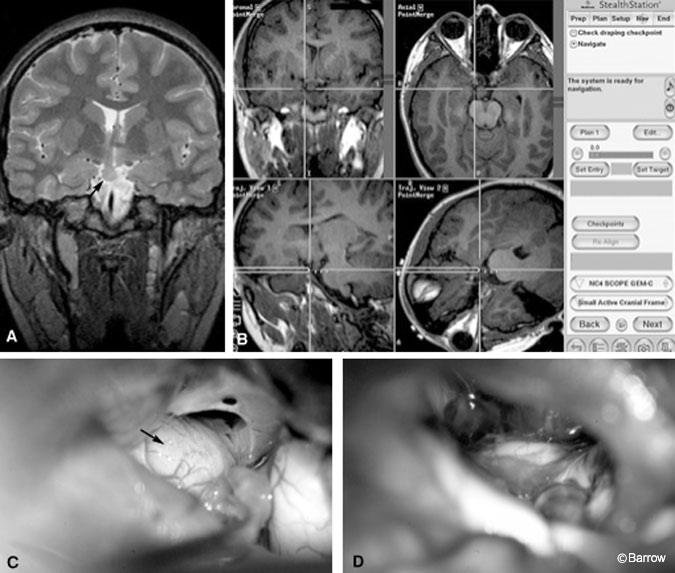
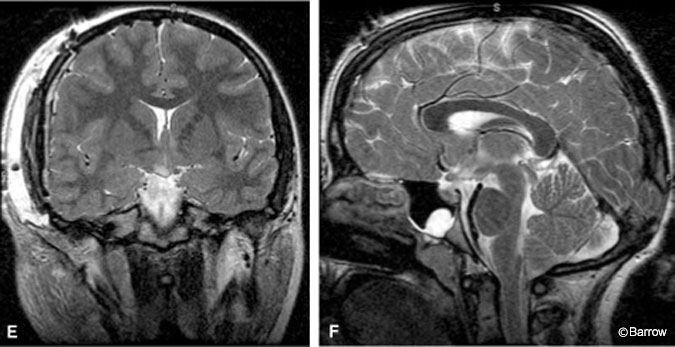
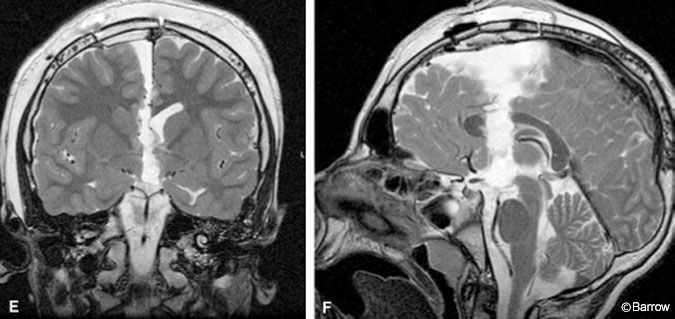
A 13-year-old girl had been diagnosed in infancy with gelastic seizures caused by a hypothalamic hamartoma. She was having four or five gelastic seizures a day and four or five grand mal seizures a week that medical therapy failed to control. She also exhibited rage behavior, and home schooling was necessary. MR imaging (Fig. 1A) verified the presence of the hypothalamic hamartoma.
Under stereotactic navigational guidance (Fig. 1B), a right modified orbitozygomatic approach was performed to resect the lesion (Fig. 1C and D). MR imaging confirmed complete resection of the lesion (Fig. 1E and F). After surgery the patient had bitemporal hemianopsia. At the patient’s 3-month follow-up examination, her parents reported that she no longer had rages or seizures and that she was able to attend a regular school. Her bitemporal hemianopsia persisted, but her memory was intact.
Transcallosal Anterior Interforniceal Approach
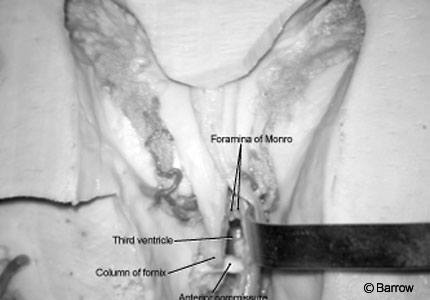
After becoming frustrated with the access provided by the pterional approach, Rosenfeld et al.[28] began operating on these lesions using a slightly more anterior interforniceal approach (Fig. 2) than the classical approach described by Apuzzo et al.[3] This variation was an attempt to remain anterior to the body of the fornix to avoid damaging memory. His initial results were rewarding, and many desperate families were referred to him from around the world.[28]
After performing the first six transcallosal procedures with Dr. Rosenfeld, we have added a few modifications that have made subsequent surgical procedures easier to perform. Our observations have shown that most of these lesions are primarily attached to the hypothalamus on one side or the other. As reported by Lawton and colleagues,[16] we have found that it is preferable to approach masses in the third and lateral ventricles via the transcallosal approach with the patient’s head in a lateral, head-up position, with the side of the lesion superior. A roll is placed under the shoulder on the side of the lesion with the head turned so that the sagittal sinus is parallel to the floor and the head is elevated 30 to 40 degrees from the table. An incision is made just behind the hairline, anterior and parallel to the coronal suture. The anteroposterior length of the craniotomy is about 5 cm. The posterior cut is just posterior and parallel to the coronal suture. The craniotomy continues about 1 cm beyond the midline sagittal suture and 3 cm below. Frameless stereotactic guidance is considered essential for this procedure.
The contralateral hemisphere, which is in the dependent position, is dissected from the midline. Care is exerted to preserve any veins that enter the sagittal sinus in the region of the coronal suture. Using frameless stereotaxy to determine the midline, the corpus callosum is opened longitudinally until a dark line indicating the midline is identified. This dark line is the superior aspect of the septum pellucidum and defines the two leaves of this structure. The line also can be visualized diaphanoscopically before performing the callosotomy by using the light source of an neuroendoscope. By shining through the corpus callosum, the light illuminates the lateral ventricles faintly. At the same time the shadow of the septum pellucidum becomes visible. This maneuver allows the surgeon to start the callosotomy over the area of the septum pellucidum.
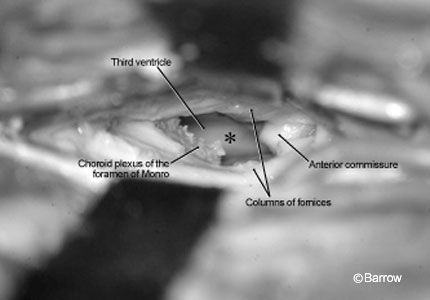
The two leaves of the septum pellucidum are dissected carefully and separated with Greenberg retractors. The dissection distracts the columns of the fornix, which are attached to the undersurface of the leaves of the septum pellucidum laterally. This opening provides access to the third ventricle from its anterior extent (where the choroid plexus defines the foramen of Monro) to the anterior commissure (Fig. 3). Immediately on entering the third ventricle, the surgeon can see the hamartoma, which appears as a lump on the ventricular floor.
The surface of the hypothalamic hamartoma is identified by the distortion of the underlying structures and by the use of frameless stereotaxy. At this point, the lesion is the same color as the ependymal surface of the remainder of the third ventricle. After it has been coagulated, the hamartoma appears gray and moist. It is removed using standard techniques. At the posterior and inferior margins of the mass, the pial surface of the interpeduncular cistern is encountered and usually opened. The lateral extent of the resection is guided by frameless stereotaxy to avoid the hypothalamus and optic radiations. For large tumors, the resection may be limited anteriorly by the optic chiasm. In some cases, it may be necessary to perform a pterional approach to remove the remaining mass. In our experience and in that of Rosenfeld, it has only been necessary to disconnect the mass laterally. The remaining anteriormost portion of the lesion causes no further problems.

Illustrative Case 2
A 10-year-old boy had experienced as many as 25 gelastic seizures a day since birth. He exhibited cognitive deficits and behavioral rages and was refractory to medical treatment. Magnetic resonance (MR) imaging showed a hypothalamic hamartoma (Fig. 4A). Under stereotactic navigational guidance (Fig.4B), a transcallosal anterior interforniceal approach was performed, and gross total resection of the lesion was achieved (Figs. 4C and D). Immediate postoperative MR imaging confirmed complete resection of the hamartoma (Fig. 4E and F). Postoperatively, the patient was lethargic for a week before recovering. At his 8-month follow-up examination, he was free of seizures. His behavioral and cognitive deficits had improved, and he no longer experienced rages. He exhibited a mild deficit in short-term memory, but his overall performance at school had improved significantly.
Neuroendoscopic Approach
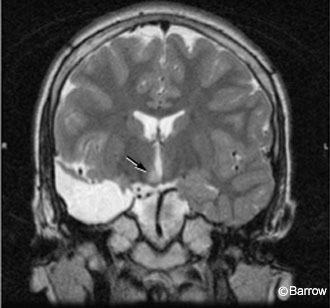
These patients rarely have enlarged ventricles. Intraventricular manipulation of the neuroendoscope is therefore difficult. Patients with small masses situated in the lateral wall of the midportion of the third ventricle are ideal candidates for resection using the neuroendoscope (Fig. 5).[1,9] We have seen only three patients who were appropriate candidates for this minimally invasive approach. Choi (Choi JU, personal communication, 2003) reported their experiences treating hypothalamic hamartomas neuroendoscopically following the principles of Delalande and Fohlen9 who believe that only the superior aspect of the mass needs to be disconnected from the surrounding hypothalamus. Choi (Choi JU, personal communication, 2003) performed endoscopic exploration on four patients and coagulated the surface of the hamartoma using a yttrium-aluminumgarnet laser (YAG) laser. Akai et al.[1] used a neuroendoscopic approach to obtain a biopsy to verify the diagnosis of hypothalamic hamartoma. Subsequently, they combined transventricular endoscopic resection with a pterional approach to resect the lesion. However, more experience with patients with intractable epilepsy is needed before the value of neuroendoscopic management of hypothalamic hamartomas can be determined.
Illustrative Case 3
An 11-year-old boy experienced the onset of gelastic seizures at the age of 6 weeks. At the age of 8 years, a hypothalamic hamartoma was diagnosed. EEG recordings localized seizures to the right temporal lobe. The boy underwent resection of his right temporal lobe, and his condition worsened. Because the hamartoma was small (Fig. 5) and the boy’s clinical course was deteriorating, the hamartoma was resected through a transcortical transventricular endoscopic approach through the foramen of Monro. Postoperatively, the patient’s seizures stopped and he was discharged home.
Other Treatment Options
Gamma Knife Radiosurgery
Gamma knife radiosurgery has been used to treat intractable seizures in a limited number of patients with hypothalamic hamartomas. This technique uses a stereotactic frame and 201 collimated cobalt-60 sources to deliver a high dose of ionizing radiation to a precisely defined target volume in a single treatment session.
Certain aspects of hypothalamic hamartomas make them appealing candidates for radiosurgical treatment. They are relatively small. They are well visualized on MR imaging, and their surgical removal may be associated with significant morbidity. Radiosurgery stops or markedly improves intractable seizures associated with mesial temporal sclerosis, cavernous malformations, and arteriovenous malformations.[24] Animal models of epilepsy also suggest that radiosurgery may markedly reduce seizure frequency without producing tissue necrosis.[19]
The primary technical difficulty in using Gamma knife radiosurgery to treat hypothalamic hamartomas is their proximity to the optic chiasm and optic tracts. Unless there is 2 to 3 mm of separation between these structures and the lesion being treated, it may be impossible to deliver a therapeutic dose to the entire hypothalamic hamartoma without exceeding a dose to the optic apparatus that could produce radiationinduced visual loss. Furthermore, 3 to 6 months and possibly longer must elapse before the effects of radiosurgery on seizure control begin.
Regis et al.[27] reported the largest series of hypothalamic hamartomas treated with Gamma knife radiosurgery. This multicenter study evaluated eight patients with drug intractable gelastic, complex partial, and generalized seizures. The patients were followed a median of 28 months (range, 12-71 months). The median dose to the margins of the hypothalamic hamartomas was 15 to 25 Gy (range, 12 to 20 Gy). Four patients became seizure free after treatment, the frequency of seizures was reduced markedly in two patients, and two patients improved moderately. All patients who became seizure free received a margin radiation dose of more than 17 Gy while those who improved received less than 13 Gy. Complete coverage was unnecessary to ensure success because the dosimetry in two seizure-free patients spared a significant portion of their lesion to avoid adjacent critical structures. Complications were limited to the onset of nondisabling poikilothermia in a single patient.
Several other centers have reported their experience with fewer patients. Unger et al.[32] treated four patients with gelastic epilepsy caused by a hypothalamic hamartoma to a margin dose of 12 to 14 Gy. All were improved but not seizure free at follow-up intervals ranging from 12 to 68 months. At the University of Pittsburgh, Kondziolka et al.[14] performed radiosurgery on two patients with intractable epilepsy and small-volume hypothalamic hamartomas. Seizures had improved in both 18 and 6 months after treatment with margin doses of 16 and 18 Gy, respectively.
The limited amount of information contained in these papers and a handful of others suggests that Gamma knife radiosurgery can decrease the frequency of seizures in most patients with gelastic epilepsy and can be curative in fewer. The likelihood of becoming seizure free seems greater after open surgical resection of hypothalamic hamartomas, but the risk of producing new neurologic deficits is considerably lower with radiosurgery. However, these conclusions are based on small numbers of patients with relatively brief follow up. More experience will be needed before the true role of radiosurgery in treating medically intractable seizures associated with hypothalamic hamartomas becomes clear.
At present we believe radiosurgery is a reasonable option for patients or families who wish a lower risk alternative to open surgical resection, particularly if the lesion is small and does not directly contact the optic chiasm. Surgery at a later date is not precluded if radiosurgery is unsuccessful. Patients who have persistent seizures after undergoing subtotal surgical resection of a hypothalamic hamartoma also may be good candidates for Gamma knife therapy. At our institution, we have followed the recommendation of Regis et al.[27] to deliver a lesion margin dose of 17 Gy or greater. If this dose cannot be delivered without exposing the optic apparatus to a dose that exceeds 8 Gy, the dosimetry is modified so that a portion of the hamartoma adjacent to critical structures receives a lower dose.
Stereotactic Radiofrequency Ablation
The stereotactic implantation of a radiofrequency source and denaturing of the hypothalamic hamartoma have been reported to eliminate epilepsy in eight patients.[12,26] This technique has promise, but we have no experience with the procedure.
Vagal Nerve Stimulation
Vagal nerve stimulation has been reported to help control seizures and to improve behavior.[23] Based on our experience, however, this technique does not appear to be efficacious for the treatment of gelastic seizures. Therefore, we believe it plays no role in the current management of gelastic seizures associated with hypothalamic hamartomas.
Conclusion
Epilepsy associated with sessile hypothalamic hamartomas is often catastrophic and precludes a normal life for patients and their family. Surgery offers these patients a better quality of life and, in many cases, the chance to live a reasonably normal life. The surgical procedures, however, are associated with significant risks and should not be undertaken for mild symptoms. They should be reserved for patients who are completely dysfunctional because of both their seizure disorder and extreme behavioral difficulties.
Not all patients with hypothalamic hamartomas are the same symptomatically or anatomically. It is essential to match the treatment with the patient. A few patients are not affected enough to justify the risks of intervention. A thorough review of the anatomic aspects of the lesion and surrounding structures is needed after the patient is identified as a surgical candidate to determine the most appropriate surgical approach for each patient.
For sessile hypothalamic hamartomas a transcallosal anterior interforniceal approach is preferred at our institution. Compared to a transcallosal anterior interforniceal approach, an orbitozygomatic approach may offer better visualization for pedunculated hypothalamic hamartomas. However, a direct comparison of both approaches is needed to clarify the particular indications associated with each approach.
Gamma knife is an interesting option because the target and necessary dosage are delineated more clearly than previously. If Gamma knife treatment is unsuccessful, it does not preclude or make subsequent surgery more difficult.
References
- Akai T, Okamoto K, Iizuka H, et al: Treatments of hamartoma with neuroendoscopic surgery and stereotactic radiosurgery: A case report. Minim Invasive Neurosurg 45:235-239, 2002
- Albright AL, Lee PA: Neurosurgical treatment of hypothalamic hamartomas causing precocious puberty. J Neurosurg 78:77-82, 1993
- Apuzzo ML, Chikovani OK, Gott PS, et al: Transcallosal, interfornicial approaches for lesions affecting the third ventricle: Surgical considerations and consequences. Neurosurgery 10: 547-554, 1982
- Arita K, Ikawa F, Kurisu K, et al: The relationship between magnetic resonance imaging findings and clinical manifestations of hypothalamic hamartoma. J Neurosurg 91:212-220, 1999
- Berkovic SF, Andermann F, Melanson D, et al: Hypothalamic hamartomas and ictal laughter: Evolution of a characteristic epileptic syndrome and diagnostic value of magnetic resonance imaging. Ann Neurol 23:429-439, 1988
- Boyko OB, Curnes JT, Oakes WJ, et al: Hamartomas of the tuber cinereum: CT, MR, and pathologic findings. AJNR Am J Neuroradiol 12:309-314, 1991
- Cascino GD, Andermann F, Berkovic SF, et al: Gelastic seizures and hypothalamic hamartomas: Evaluation of patients undergoing chronic intracranial EEG monitoring and outcome of surgical treatment. Neurology 43:747-750, 1993
- Debeneix C, Bourgeois M, Trivin C, et al: Hypothalamic hamartoma: Comparison of clinical presentation and magnetic resonance images. Horm Res 56:12-18, 2001
- Delalande O, Fohlen M: Disconnecting surgical treatment of hypothalamic hamartoma in children and adults with refractory epilepsy and proposal of a new classification. Neurol Med Chir (Tokyo) 43:61-68, 2003
- Feiz-Erfan I, Ferreira MAT, Rekate HL, et al: The utility of skull base approaches for the resection of hypothalamic hamartomas causing gelastic seizures in children (abstract). Skull Base: An Interdisciplinary Approach 12 (Suppl 1):12, 2002
- Frattali CM, Liow K, Craig GH, et al: Cognitive deficits in children with gelastic seizures and hypothalamic hamartoma. Neurology 57:43-46, 2001
- Fujimoto Y, Kato A, Saitoh Y, et al: Stereotactic radiofrequency ablation for sessile hypothalamic hamartoma with an image fusion technique. Acta Neurochir (Wien) 145:697-700, 2003
- Jung H, Neumaier Probst E, Hauffa BP, et al: Association of morphological characteristics with precocious puberty and/or gelastic seizures in hypothalamic hamartoma. J Clin Endocrinol Metab 88:4590-4595, 2003
- Kondziolka D, Singhal D, Niranjan A, et al: Stereotactic radiosurgery for epilepsy and movement disorders, in Pollock BG (ed): Contemporary Stereotactic Radiosurgery: Technique and Evaluation. Elmsford, NY: Blackwell Futura, 2002, pp 327-345
- Kramer U, Spector S, Nasser W, et al: Surgical treatment of hypothalamic hamartoma and refractory seizures: A case report and review of the literature. Pediatr Neurosurg 34:40-42, 2001
- Lawton MT, Golfinos JG, Spetzler RF: The contralateral transcallosal approach: Experience with 32 patients. Neurosurgery 39:729-734, 1996
- Likavec AM, Dickerman RD, Heiss JD, et al: Retrospective analysis of surgical treatment outcomes for gelastic seizures: A review of the literature. Seizure 9:204-207, 2000
- Luo S, Li C, Ma Z, et al: Microsurgical treatment for hypothalamic hamartoma in children with precocious puberty. Surg Neurol 57:356-362, 2002
- Maesawa S, Kondziolka D, Dixon CE, et al: Subnecrotic stereotactic radiosurgery controlling epilepsy produced by kainic acid injection in rats. J Neurosurg 93:1033-1040, 2000
- Mahachoklertwattana P, Kaplan SL, Grumbach MM: The luteinizing hormone-releasing hormone-secreting hypothalamic hamartoma is a congenital malformation: Natural history. J Clin Endocrinol Metab 77:118-124, 1993
- Mottolese C, Stan H, Bret P, et al: Hypothalamic hamartoma: The role of surgery in a series of eight patients. Childs Nerv Syst 17:229-238, 2001
- Mullatti N, Selway R, Nashef L, et al: The clinical spectrum of epilepsy in children and adults with hypothalamic hamartoma. Epilepsia 44:1310-1319, 2003
- Murphy JV, Wheless JW, Schmoll CM: Left vagal nerve stimulation in six patients with hypothalamic hamartomas. Pediatr Neurol 23:167-168, 2000
- Niranjan A, Lunsford LD: Radiosurgery: Where we were, are, and may be in the third millennium. Neurosurgery 46:531-543, 2000
- Northfield DW, Russell DS: Pubertas praecox due to hypothalamic hamartoma: Report of two cases surviving surgical removal of the tumour. J Neurol Neurosurg Psychiatry 30:166-173, 1967
- Parrent AG: Stereotactic radiofrequency ablation for the treatment of gelastic seizures associated with hypothalamic hamartoma. Case report. J Neurosurg 91:881-884, 1999
- Regis J, Bartolomei F, de Toffol B, et al: Gamma knife surgery for epilepsy related to hypothalamic hamartomas. Neurosurgery 47:1343-1352, 2000
- Rosenfeld JV, Harvey AS, Wrennall J, et al: Transcallosal resection of hypothalamic hamartomas, with control of seizures, in children with gelastic epilepsy. Neurosurgery 48:108-118, 2001
- Siomin V, Spektor S, Beni-Adani L, et al: Application of the orbito-cranial approach in pediatric neurosurgery. Childs Nerv Syst 17:612-617, 2001
- Stewart L, Steinbok P, Daaboul J: Role of surgical resection in the treatment of hypothalamic hamartomas causing precocious puberty. Report of six cases. J Neurosurg 88:340-345, 1998
- Striano S, Meo R, Bilo L, et al: Gelastic epilepsy: Symptomatic and cryptogenic cases. Epilepsia 40:294-302, 1999
- Unger F, Schrottner O, Feichtinger M, et al: Stereotactic radiosurgery for hypothalamic hamartomas. Acta Neurochir Suppl 84:57-63, 2002
- Valdueza JM, Cristante L, Dammann O, et al: Hypothalamic hamartomas: With special reference to gelastic epilepsy and surgery. Neurosurgery 34:949-958, 1994
- Weissenberger AA, Dell ML, Liow K, et al: Aggression and psychiatric comorbidity in children with hypothalamic hamartomas and their unaffected siblings. J Am Acad Child Adolesc Psychiatry 40:696-703, 2001