


Headache in Autosomal Dominant Polycystic Kidney Disease Due to Spontaneous Vertebral Artery Dissection
Wouter I. Schievink, MD*
Cameron G. McDougall, MD
Robert F. Spetzler, MD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
*Current Address: Cedars-Sinai Neurosurgical Institute, Los Angeles, California
Abstract
Autosomal dominant polycystic kidney disease (ADPKD), a heritable connective tissue disorder, is well known for its association with intracranial aneurysms. Spontaneous dissection of a vertebral artery, however, is rarely reported as a complication of ADPKD. A 32-year-old woman with ADPKD suffered a subarachnoid hemorrhage from a ruptured saccular aneurysm of the middle cerebral artery. Angiography showed an extracranial dissection of the left vertebral artery. At age 30, she had experienced left-sided neck pain and an occipital headache. At that time a subarachnoid hemorrhage had been ruled out, but no cause for her headache was found. ADPKD is associated with a generalized arteriopathy. In a patient with ADPKD and a new headache, the index of suspicion should be high not only for an intracranial aneurysm but also for a spontaneous cervical artery dissection.
Key Words : aneurysm, arterial dissection, autosomal dominant polycystic kidney disease, subarachnoid hemorrhage, vertebral artery
Autosomal dominant polycystic kidney disease (ADPKD) is the most common monogenetic disorder in humans. Its prevalence is between 1 in 400 to 1000 persons, and it accounts for 8 to 10% of end stage renal failure worldwide.3 Numerous extrarenal complications of ADPKD have been reported. Many affect a variety of connective tissues, and ADPKD should be included among the heritable connective tissue disorders.3,10,13 We report a patient with ADPKD and a spontaneous dissection of the extracranial vertebral artery, a rarely reported complication of ADPKD that is important to recognize in the differential diagnosis of unusual headaches in patients with ADPKD.
Case Report
On August 19, 1997, a 32-year-old woman developed a sudden and severe headache and she collapsed. Her medical history was significant for ADPKD associated with polycystic liver disease, which had been diagnosed when she was 22 years old. Her sister and father also had ADPKD. Arterial hypertension was first noted at age 24, but she refused medical treatment. At age 30, she complained of a sudden and unusual neck pain on the left side that later involved the occiput. The next day she was seen in the Emergency Department where a diagnosis of aneurysmal subarachnoid hemorrhage was strongly considered. However, her computed tomography (CT) scan and cerebrospinal fluid (CSF) examination were normal. No family member was known to have had an intracranial hemorrhage, aneurysm, or stroke at a young age.
Upon arrival in our Emergency Department, her blood pressure was 200/105 mm Hg and her heart rate was 100 beats/minute. Her Glasgow Coma Scale score was 6, and her World Federation of Neurological Surgeons grade was V. Her right pupil was enlarged and sluggishly reactive to light, and she had a left hemiparesis. A CT scan showed a large hematoma in the right temporal lobe and intraventricular hemorrhage. The right pupil became fixed and dilated and a ventriculostomy was placed.
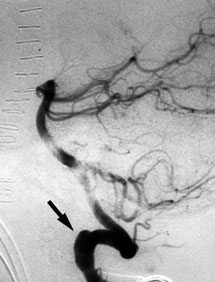
The patient underwent emergency surgery without preoperative angiography. The hematoma was evacuated, and an approximately 1-cm, ruptured, saccular aneurysm of the right middle cerebral artery (MCA) was clipped. Postoperative angiography showed an extracranial dissection of the left vertebral artery at C1-C2 (Fig. 1), a 2-mm aneurysm on the right supraclinoid carotid artery, and small bulbous dilatations on the left MCA bifurcation and tip of the basilar artery. Obliteration of the ruptured aneurysm on the right MCA was confirmed. After surgery, the patient gradually improved. She is undergoing rehabilitation.
Discussion
Intracranial aneurysms are the most well-known extrarenal manifestations of ADPKD, and patients with ADPKD and a new headache (with or without neurological signs or symptoms) should be suspected of a symptomatic intracranial aneurysm.15 The index of suspicion, however, should also be high for hypertensive cerebral hemorrhage12 and intracranial hypotension caused by a CSF leak from spinal meningeal diverticula.14 Our case suggests that patients with ADPKD also are at increased risk for spontaneous cervical artery dissections. When our patient developed neck pain and an occipital headache, a subarachnoid hemorrhage (SAH) was ruled out. A vertebral artery dissection, however, was not considered and remained undiagnosed until she underwent angiography 2 years later for the aneurysmal SAH. The association of cervical artery dissections and intracranial aneurysms is not uncommon, especially in the setting of a generalized arteriopathy.13
Numerous cardiovascular manifestations of ADPKD have been reported, including mitral valve prolapse, coronary artery aneurysms, saccular intracranial aneurysms, intracranial arterial dolichoectasia, and spontaneous dissections involving intracranial arteries and the thoracic aorta.1-3,6,9,11,13,15,16 Three patients with ADPKD and cervical artery dissections have been reported. In two patients the dissection was traumatic.2,5 The other patient had also suffered three aortic dissections from an unusual, overlapping familial connective tissue disorder (Table 1).7,17 The frequency of cervical artery dissection in ADPKD is unknown. Of 93 ADPKD patients screened for asymptomatic intracranial aneurysms with magnetic resonance angiography, three patients had subcranial aneurysms of the internal carotid artery possibly caused by a dissection.11
Our case provides further evidence for the presence of generalized arteriopathy in ADPKD. Although the exact mechanisms have not yet been elucidated, this arteriopathy is likely related to abnormal function of the proteins polycystin-1 and polycystin-2, which are encoded by the ADPKD genes.8,10 The polycystins are integral membrane proteins containing multiple extracellular domains that may play a role in maintaining the structural integrity of connective tissues including the vessel wall. Polycystin is strongly expressed in the vascular smooth muscle of large and medium-sized arteries, including cervical and intracranial arteries.4
References
- Adubofour K, Sidaway L, Glatter T: Coronary artery aneurysms in association with adult polycystic kidney disease. Am Heart J 127:1411-1413, 1994
- Chapman AB, Rubinstein D, Hughes R, et al: Intracranial aneurysms in autosomal dominant polycystic kidney disease. N Engl J Med 327:916-920, 1992
- Gabow PA: Autosomal dominant polycystic kidney disease. N Engl J Med 329:332-342, 1993
- Griffin MD, Torres VE, Grande JP, et al: Vascular expression of polycystin in ADPKD and control subjects. J Am Soc Nephrol 8:616-626, 1997
- Guthrie W, Maclean H: Dissecting aneuryms of arteries other than the aorta. J Pathol 108:219-235, 1972
- Kulla L, Deymeer F, Smith TW, et al: Intracranial dissecting and saccular aneurysms in polycystic kidney disease. Arch Neurol 39:776-778, 1982
- Larranaga J, Rutecki GW, Whittier FC: Spontaneous vertebral artery dissection as a complication of autosomal dominant polycystic kidney disease. Am J Kidney Dis 25:70-74, 1995
- Ong AC, Harris PC: Molecular basis of renal cyst formation—one hit or two? Lancet 349:1039-1040, 1997
- Paynter HE, Parnham A, Feest TG, et al: Thoracic aortic dissection complicating autosomal dominant polycystic kidney disease.Nephrol Dial Transplant 12:1711-1713, 1997
- Perrone RD: Extrarenal manifestations of ADPKD. Kidney Int 51:2022-2036, 1997
- Ruggieri PM, Poulos N, Masaryk TJ, et al: Occult intracranial aneurysms in polycystic kidney disease: Screening with MR angiography. Radiology 191:33-39, 1994
- Ryu SJ: Intracranial hemorrhage in patients with polycystic kidney disease. Stroke 21:291-294, 1990
- Schievink WI, Michels VV, Piepgras DG: Neurovascular manifestations of heritable connective tissue disorders. A review. Stroke 25:889-903, 1994
- Schievink WI, Torres VE: Spinal meningeal diverticula in autosomal dominant polycystic kidney disease. Lancet 349:1223-1224, 1997
- Schievink WI, Torres VE, Piepgras DG, et al: Saccular intracranial aneurysms in autosomal dominant polycystic kidney disease. J Am Soc Nephrol 3:88-95, 1992
- Schievink WI, Torres VE, Wiebers DO, et al: Intracranial arterial dolichoestasia in autosomal dominant polycystic kidney disease. J Am Soc Nephrol 9:1298-1303, 1997
- Somlo S, Rutecki G, Giuffra LA, et al: A kindred exhibiting cosegregation of an overlap connective tissue disorder and the chromosome 16 linked form of autosomal dominant polycystic kidney disease. J Am Soc Nephrol 4:1371-1378, 1993