


The BNI Screen for Children: Rationale and Initial Validation Studies*
Author
George P. Prigatano, PhD
Division of Neurology, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center
*This article was made possible by funds from the Newsome Chair in Neuropsychology.
Abstract
This article introduces the BNI Screen for Higher Cerebral Functions for School-Age Children (BNIS-C). The rationale that guided the development of this screening test and the initial validation findings are presented. The test appears to be sensitive to age effects (as intended) and to differentiate children with unequivocal brain dysfunction from children without brain dysfunction who are performing normally in public schools.
Key Words: BNIS-C, children, higher cerebral function, normative data, validation studies
Forty years ago, Diller and Birch[1] outlined the numerous problems encountered in the neuropsychological evaluation of children. They noted that the following variables can influence performance on various psychological measures: (1) age at time of brain insult, (2) age at time of neuropsychological examination, (3) locus and severity of brain injury, (4) type of brain insult, and (5) duration or chronicity of brain insult. They also observed that “. . . in the main, psychological tests are not developmentally oriented and the information they supply is discontinuous from age to age” (p 27).[1] They emphasized that a “wide variety of stimulus situations” (p 29) should be used when examining such children and suggested the use of projective measures, memory and learning tasks, speed and accuracy of perceptual and motor skills, and various problem-solving tasks.
Clinically, the neuropsychological examination of children with known or suspected brain disorders is likely to yield optimal information when the following conditions are met. (1) The examination procedures should hold the interest of the child because their motivation to perform can greatly influence findings. Thus, the test items must be socially and culturally meaningful to children at a given age. (2) The various neuropsychological test items should be developmentally sensitive. That is, while the test items or requests may remain the same, different levels of performance may be obtained at different stages of development. (3) The neuropsychological test findings should reliably distinguish children with known brain disorders from children without such disorders. (4) The neuropsychological test items should help elucidate the interactive effects of known brain lesions and the developmental problem-solving capacities of children. This requirement is perhaps the most demanding. (5) The scope of neuropsychological test items should be broad to assess many possible disturbances, yet the test should be time efficient. Several hours of testing often produce fatigue and boredom in both children and examiners.
Although various testing procedures are available,[2] appreciation has been growing that certain basic dimensions should be assessed during the clinical neuropsychological examination of adults and children:[6] speech and language functions, perceptual skills (auditory, visual, and tactual), attention and concentration skills, learning and memory capacities, intellectual level and executive functions, speed of new learning, speed and coordination of simple motor responses, emotional and motivational characteristics, and self-awareness of functioning and judgments concerning psychosocial implications. Although no test can yet assess all of these dimensions rapidly and thoroughly, 8 screening tests should provide a broad enough sample of the behavior and thought processes of adults or children to permit initial inferences about their capacities on each of these dimensions.
The BNI Screen (BNIS) for Higher Cerebral Functions was developed to obtain such information in adults.[3-5,9] Clinical and research experience with that test was used to develop the BNIS for School-Age Children (BNIS-C). Although children are clearly not “little adults,” their neuropsychological abilities form a continuum from their early school years, throughout adolescence, and, ultimately, into adulthood. At each stage, language functions, concentration, attention, memory, problem-solving, and emotional and motivational characteristics must be assessed. The performance of adults with and without brain dysfunction was analyzed to identify items that could potentially reveal something about children’s higher integrative brain functions. This initial report presents the descriptive data of the first 50 children studied in public schools and compares their mean performance to that of children with known brain disorders.
Materials and Methods
Rationale Underlying the BNIS-C
The BNIS-C is a “downward” extension of the BNIS used for adults. Preliminary observations suggested that the downward extension could be meaningfully applied to school-aged children (i.e., 7 to 14 years old). The types of items used on the BNIS appeared to need substantial alterations for preschool children. Consequently, this group was not included in this standardization study.
As with the BNIS, the BNIS-C was developed with the concept that most normal children would successfully perform most of the tasks presented to them. Obviously, a child’s developmental stage, level of intelligence, and educational experience would influence performance on certain tasks (e.g., tests of arithmetic reasoning).
An empirical approach was used to determine the level and pattern of performance that could be expected from children who were 7, 8, 9, 10, 11, 12, 13, and 14 years old. The standardization research protocol sought to examine 20 children at each age level (10 males, 10 females) who were attending public school and who required no special assistance. Ultimately, the total sample size used for standardization will be 180 children. Children diagnosed as having a learning disability or as needing a resource class to meet academic requirements were excluded from this sample.
Other neuropsychological measures were also administered to stratify the children according to level of intelligence when interpreting their performance on the BNIS-C. The Vocabulary and Block Design subtests of the Wechsler Intelligence Scale for Children-4th edition (WISC-IV) 11 were administered to each child. Children with age adjusted scale scores of 8 or higher on both measures were considered to have normal to above normal intelligence. In the standardization study of the WISC-IV, the mean scale score is 10 with a standard deviation (SD) of 3. The intelligence of children who score 7 or below on one or both measures is considered to be below average. Thus the performance on the BNIS-C of children with normal to above normal intelligence and those with below normal intelligence could be assessed meaningfully at different age ranges.
Test Materials
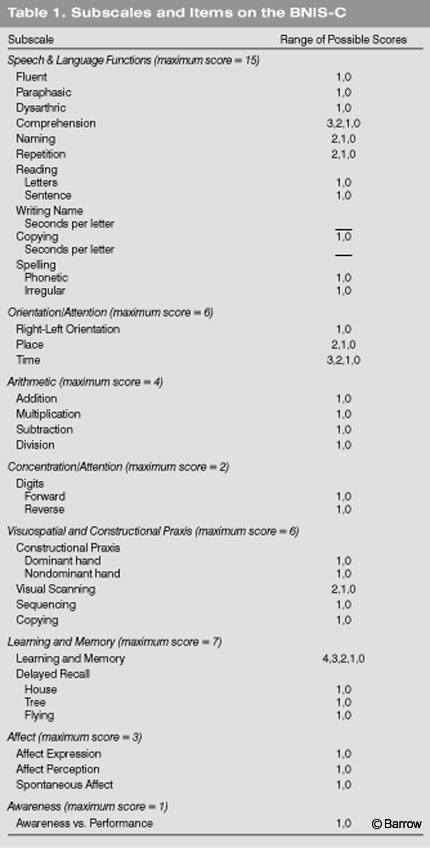
The manual of the BNIS-C details the test items and how they are administered.[7] “Prescreening” items allow the examiner to rate a child’s readiness to be examined. Level of consciousness/alertness, basic language function, and level of cooperation are assessed. Various subtests are then administered to assess childrens’ functioning in the eight domains represented on the subscales of the BNIS: speech and language function, orientation, arithmetic, concentration/attention, visuospatial and constructional practice, learning and memory, affect, and awareness (Table 1). The prescreening items plus the total of the subscale items constitute the Total score, which equals 50 points.

Initial Validation Studies
The first step in validating the BNIS-C was to obtain BNIS-C scores from school-age children to determine if the test is “developmentally sensitive.” That level of performance on the BNIS-C increases as a function of age is the clearest indication that the test is developmentally sensitive.
The second step in this initial validation study was to determine if the mean level of performance on the BNIS-C would be reliably different in children with and without brain dysfunction. It was predicted that children with brain dysfunction would perform at a lower level than nonbrain dysfunctional children when their ages were comparable.
Study Participants
Fifty children (44% males, 56% females) from public schools in Maricopa County have been administered the BNIS-C. Their mean age was 10.5 years (range, 7 to 14 years as the standardization protocol required; SD= 2.05). All children were functioning normally in public school environments. They neither attended special education classes nor required resource classes.
Twenty-one children (61% males, 39% females) with unequivocal brain dysfunction were also studied and compared to the normative sample. Their mean age was 10.4 years (SD= 2.57; range, 7 to 14 years). Fourteen children had a history of moderately severe to severe TBI as classified by the Glasgow Coma Scale and neuroimaging findings. All children had sustained their injury at least 1 year before the time of testing. Five children with a history of seizure disorders associated with a hypothalamic hamartoma were examined before surgery. Their level of intelligence was normal to below normal, but none were described as demonstrating mental retardation on tests of intelligence. Two other children were also studied. One child had a history of hydrocephalus from birth. The second had a glioma involving the left parietal lobe.
The difference in the mean age of the children with known brain dysfunction and that of the children with no known brain dysfunction who were performing adequately in the public school environment was not a statistically reliable difference (t =.620, df =69, p =.53). The percentage of males and females in the two groups was comparable.
Test Procedures
The BNIS-C, selected subtests of the WISC-IV,[11] the Halstead Finger-Tapping Test, and the BNI adaptation of the Fuld Object Memory Test[2] were administered to each child. Only data from the BNIS-C scores and the Vocabulary and Block Design subtests of the WISC-IV are discussed below.
Examiners
The tests were administered by a board-certified clinical neuropsychologist, a resident in clinical neuropsychology, or graduate students in psychology specifically trained to administer psychometric tests. Five examiners collected these data (see Acknowledgments).
Statistical Procedures
Descriptive statistics were calculated for the performance of children at different age ranges. Means and SDs were calculated for each age from 7 to 14. In addition, Students’ t-tests were used to compare mean differences in the performances of normal children and children with brain dysfunction. When applicable, t-tests for samples demonstrating unequal variance were conducted.
Results
Initial Normative Data
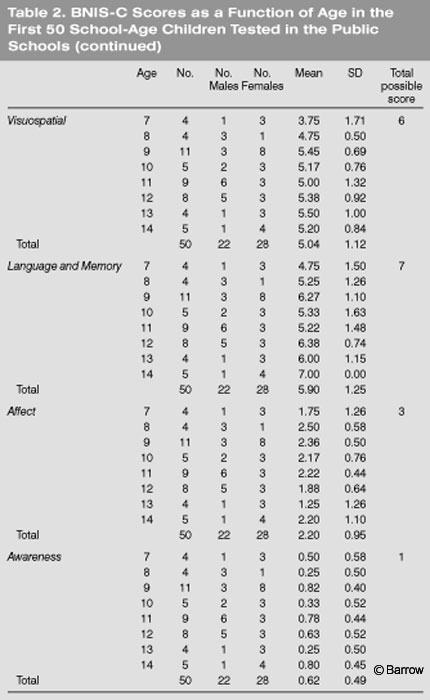
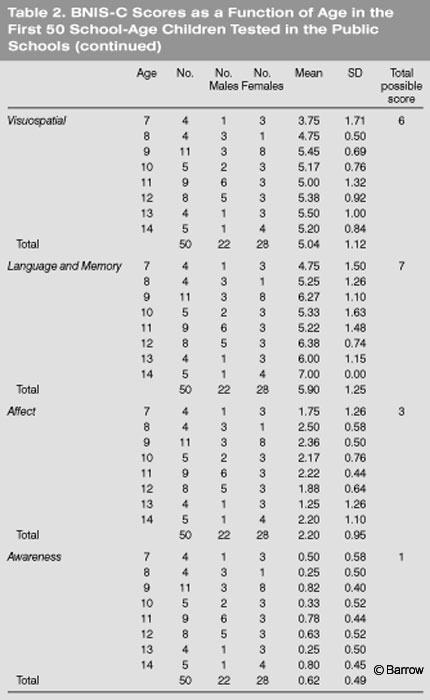
Table 2 lists the BNIS-C Total scores and the various subtest scores obtained in children from public schools. The mean Total score for the 7-year-old children (n =4) was 35.25 (of 50 points). The mean Total score of the 8-year-old children was higher at 41 points. Between the ages of 9 and 13, the mean scores appeared to cluster between 44 and 46 points. By the age of 14 years (n =5), the mean score was 46.6 points. Although the sample sizes are too small to draw firm conclusions, a developmental trend appears to be present.

Some subtest scores showed a strong linear developmental trend while others did not. For example, a stepwise function appeared to exist for orientation. At 7 and 8 years old, children did not obtain a perfect or near perfect score (6 points). At the age of 9 years and older, however, the scores approached maximum on this subtest. As would be expected, however, arithmetic and language functions tended to be linear. Ultimately, a large sample will be needed to determine the normal range for each subtest for each age.
Children with average to above average intelligence tended to perform better on the BNIS-C than children whose IQ estimates were below average (Table 3). At the age of 7 years, the mean score of the four children with normal intelligence was 35.25 (SD = 4.27). At the age of 8 years, the mean score of children with normal intelligence was 42.0 (SD=4.55). The mean scores of children between 9 and 12 years old ranged from 44 to 47 points. The mean score of both the 13 and 14 year old children was 48. The rationale underlying the BNIS-C requires older normal children to obtain a near perfect performance.
These initial data suggest a “stepwise” function between total score and age in the children with normal intelligence. The mean score appears to increase between the ages of 7 and 8 years. By the age 9 years, the score then plateaus until about the age of 12 years. By the ages of 13 and 14 years, performance almost reaches a “perfect” score (i.e., 48 of 50 points). If supported with a larger sample size, this observation will be important in the neuropsychological screening for higher cerebral functioning in children.

Performance of Children with Brain Dysfunction
The BNIS-C total score for the two groups of children was significantly different (t =3.33, df =69, p =.003) with the brain dysfunctional children having a lower mean score (Table 4). The Vocabulary score on the WISCIV tended to be slightly higher in the normal group, but the differences between the two groups on both the Vocabulary and Block Design subtests did not reach statistical significance. Thus, in this small sample, performance on the BNIS-C differentiated the two groups while their performance on the verbal and nonverbal subscales of the WISC-IV did not.
Discussion
The present data provide tentative support for two hypotheses regarding the BNIS-C. First, the BNIS-C Total score appears to be developmentally sensitive: Older children obtained higher scores on the test. A larger sample size is needed to draw firm conclusions about how age influences performance on the BNIS-C. The initial findings, however, support the proposition that this test is developmentally sensitive.
Second, the Total score on the BNIS-C reliably differentiated children with known brain dysfunction from the normal control children. The BNIS-C therefore appears useful as a brief screening test for children with brain dysfunction. Larger sample sizes will yield accurate estimates of the sensitivity and specificity of the BNIS-C.
The pattern of the normal children’s performance at different ages was informative. The effects of age did not appear to be linear on all dimensions of the BNIS-C. On some dimensions, such as the Total score, the level of performance appeared to be a graded function of age. Between the ages of 7 and 8 years, the level of performance “jumped” substantially. As more children are studied, a step-wise relationship between age and performance may emerge. After a certain age, children may perform at equal levels on different dimensions. This observation awaits further empirical support. Such a finding, however, would be consistent with the literature that focuses on patterns of cognitive development in school-age children.[10]
An extremely important question is how different types of brain injuries affect performance of children at different ages on the BNIS-C. Understanding the interaction between age and brain injury on neuropsychological performance is a key issue that neuropsychological examiners and neurorehabilitation specialists need to address. Such a demanding task, however, requires that many different types of children be examined at different age ranges.
Acknowledgments
The author thanks Kristen Kirlin, PhD; Camea Gagliardi, MEd; Saurabh Gupta; and Jennifer Sand for their help in data collection. Susan Borgaro, PhD; Camea Gagliardi, MEd; and Saurabh Gupta also helped in the statistical analysis of the data. The author thanks the Creighton Public School District and the children and families who participated in the first portion of the standardization study of the BNIS-C.
References
- Diller L, Birch HG: Psychological evaluation of children with cerebral damage, in Birch HG (ed): Brain Damage in Children: The Biological and Social Aspects. New York: Williams and Wilkins, 1964, pp 27-43
- Lezak MD: Neuropsychological Assessment. New York: Oxford University, 1995
- Prigatano GP: BNI Screen for Higher Cerebral Functions: Rationale and initial validation. BNI Quarterly 7(1):2-9, 1991
- Prigatano GP, Amin K, Rosenstein LD: Validity studies on the BNI Screen for Higher Cerebral Functions. BNI Quarterly 9(1):2-9, 1993
- Prigatano GP, Amin K, Rosenstein LD: Administration and Scoring Manual for the BNI Screen for Higher Cerebral Functions. Phoenix, AZ: Barrow Neurological Institute, 1995
- Prigatano GP, Zigler LY, Rosenstein LD: The clinical neuropsychological examination: Scope, cost, and healthcare value, in Prigatano GP, Pliskin (eds): Clinical Neuropsychology and Cost Outcome Research. New York: Psychology Press, 2003, pp 15-36
- Prigatano GP, Gagliardi CJ: BNI Screen for Higher Cerebral Functions in School Age Children: A Manual for Administration and Scoring. Phoenix, AZ: Barrow Neurological Institute, in press
- Reitan RM: Theoretical and methodological bases of the Halstead-Reitan Neuropsychological Test Battery, in Grant I, Adams KM (eds): Neuropsychological Assessment of Neuropsychiatric Disorders. New York: Oxford University Press, 1986, pp 3-30
- Rosenstein LD, Prigatano GP, Amin K: Reliability studies for the BNI Screen for Higher Cerebral Functions. BNI Quarterly 8(3):24-28, 1992
- Scarr S, Weinberg RA, Levine A: Understanding Development. New York: Harcourt Brace Jovanovich, 1986
- Wechsler D: Wechsler Intelligence Scale for Children. Administration and Scoring Manual. San Antonio, Texas: The Psychological Corporation, 2003
{kind=link}