Top Seven of Seven Series – 2022
While Dr. Lawton takes hiatus a from operating this week to enjoy some spring break skiing, we will be counting down the top seven episodes of Seven Series from 2022. Follow along as Dr. Lawton revisits his most popular videos in the series from last year and offers a reflection on each.
#7 – Far Lateral Craniotomy for Resection of a Foramen Magnum Meningioma
It’s Spring Break and I’m skiing. This week, because I’m not operating, we’ll revisit the Top Seven of Seven Series from 2022. So here we go with #7: This foramen magnum meningioma is the only tumor in the batch, and shows that open vascular skills cross over to tumors and can help cerebrovascular surgeons fill the gap from decreasing aneurysm cases.
Original Caption: Foramen magnum meningiomas wrap themselves around the vertebral artery, PICA, lower cranial nerves, and distort the medulla. These skull base tumors require good strategy (devascularize, debulk, dissect) and are the perfect application of the vascular neurosurgeon’s skillset…
Stay tuned as we reveal a new installment every day this week!
#6: Proximal Clip Occlusion of Recurrent Basilar Quadrification Aneurysm after Treatment with WEB Device
There’s a special pleasure in operating on failed endovascular cases. These devices look surreal from the subarachnoid vantage point and it’s always fun to save the day when the aneurysm recurs, as with this compacted WEB device in a basilar aneurysm.
Original Caption: Although endovascular technology advances fast and flow diverters are promising, new isn’t always better. This WEB device compacted and the aneurysm recurred – a reminder to critically evaluate new devices before abandoning tried-and-true open surgical techniques…
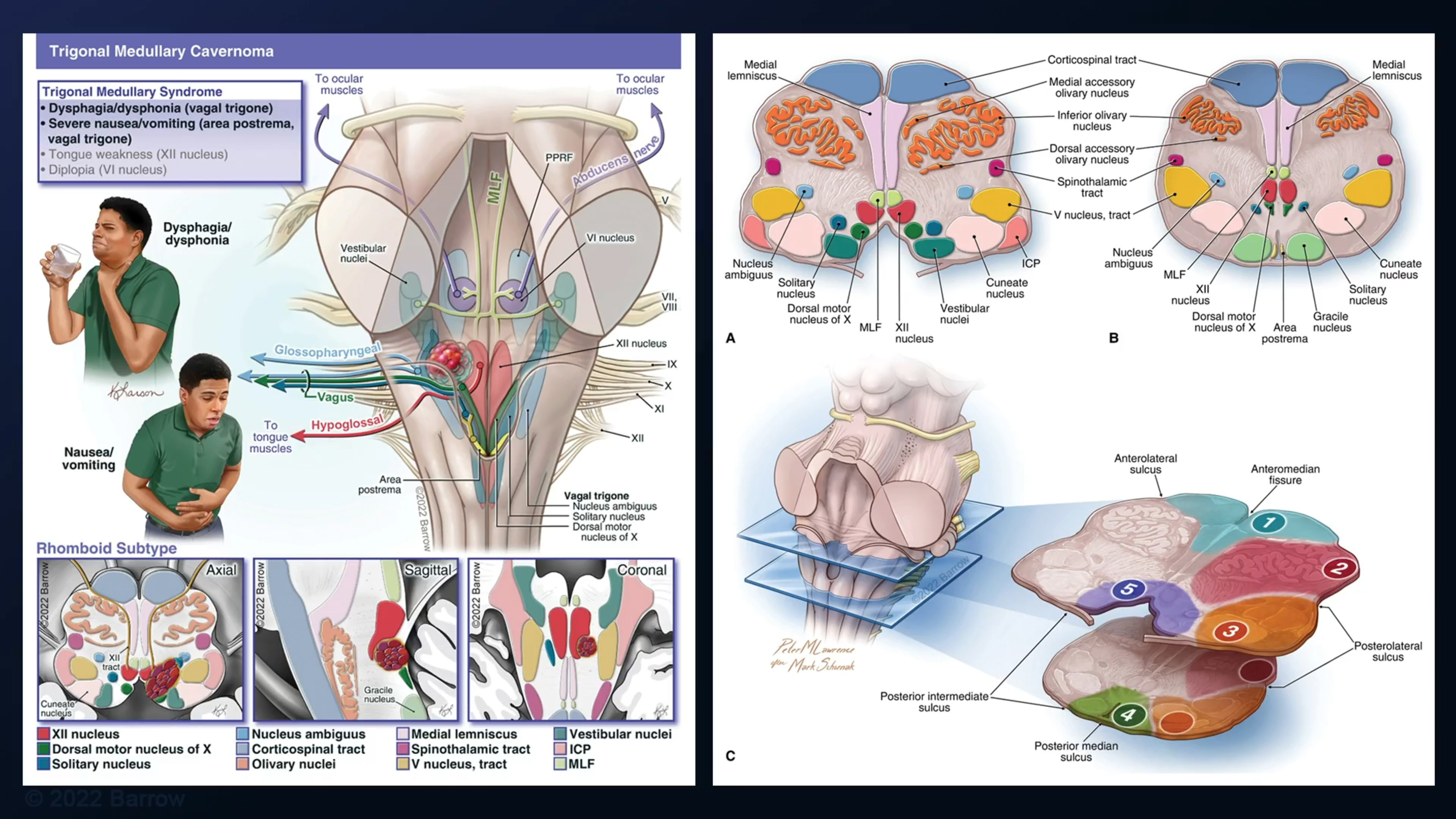
#5: Microsurgical Resection of an Inferior Medullary Cavernous Malformation
It has been a big year with the release of the taxonomy for brainstem cavernous malformations in Seven Cavernomas. Classification systems help us understand the variety of pathology and lead us to correct management decisions and good patient outcomes. This is especially true for cavernomas.
Original Caption: Gracile medullary cavernomas lie in or near midline, outside 4th ventricle, below obex, whereas trigonal medullary cavernomas lie inside 4th ventricle, on the floor, above obex. Subtonsillar triangle opens the operative corridor and posterior median sulcus is your safe entry zone.
#4: Pterional Craniotomy and Transsylvian-Transinsular Approach for Resection of Insular Lateral Thalamic Cavernous Malformation
If there’s one skill I would want every neurosurgeon to master, it’s splitting the Sylvian fissure. When you open this corridor cleanly, it takes you to important places in the brain and lets you tackle so many lesions – aneurysms, AVMs, tumors, in this case, thalamic cavernomas.
Original Caption: The “quick shot” approach through Sylvian fissure/operculum is a limited, posterior Sylvian fissure split that exposes distal M2 segments and long gyrus of the insula for transinsular resection of a giant, lateral thalamic cavernoma – minimally invasive and fast.
#3: Suboccipital Transventricular Resection of a Trigonal Medullary Cavernous Malformation
I dread arriving at the pial surface of a brainstem cavernous malformation and seeing no sign of it. You must rely on knowledge of safe entry zones and take that plunge. Is there anything more satisfying than hitting that pocket of liquified blood and knowing that you’ve arrived?
Original Caption: “Calamus scriptorius,” Latin for nib or point of a fountain pen, describes the reedlike inferior 4th ventricular floor. Trigonal medullary cavernomas sit here. The vallecular triangle, one of the 14 brainstem cavernoma triangles, is opened to access the lesion.
#2: Clip Reconstruction of a Posterior Inferior Cerebellar Artery Aneurysm with Anterograde Fenestration Tube
How can you not love the far lateral approach for a PICA aneurysm? It’s a beautiful combination of skull base surgery, posterior fossa anatomy, triangles amongst cranial nerves, and complex clipping techniques. No wonder it’s #2.
Original Caption: Ever heard of an anterograde fenestration tube? In this case, 3 stacked fenestrated clips encircle the posterior inferior cerebellar artery to close the PICA aneurysm neck and maintain parent artery patency. The tube even transmits a perforator with PICA. #Clippology
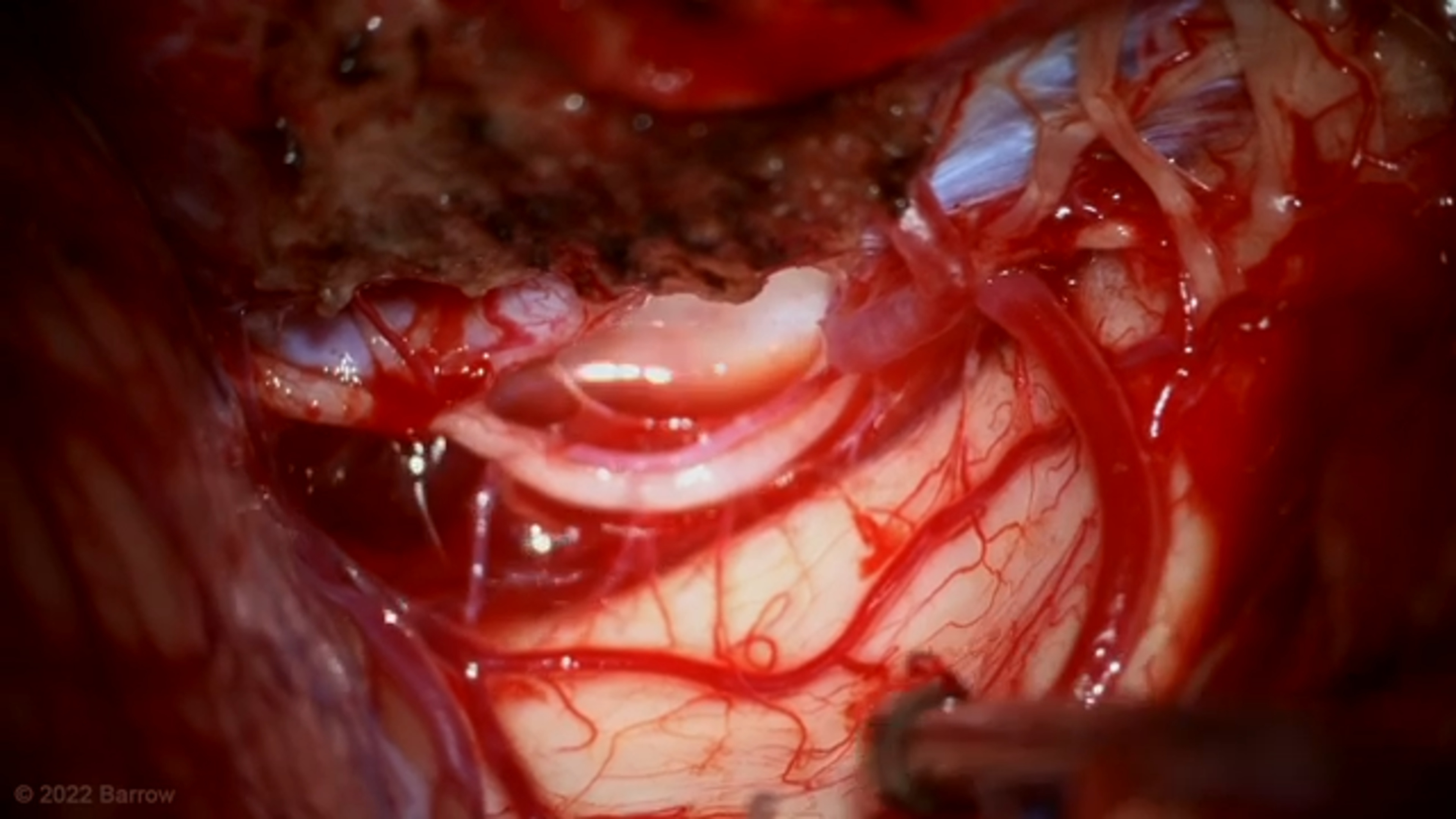
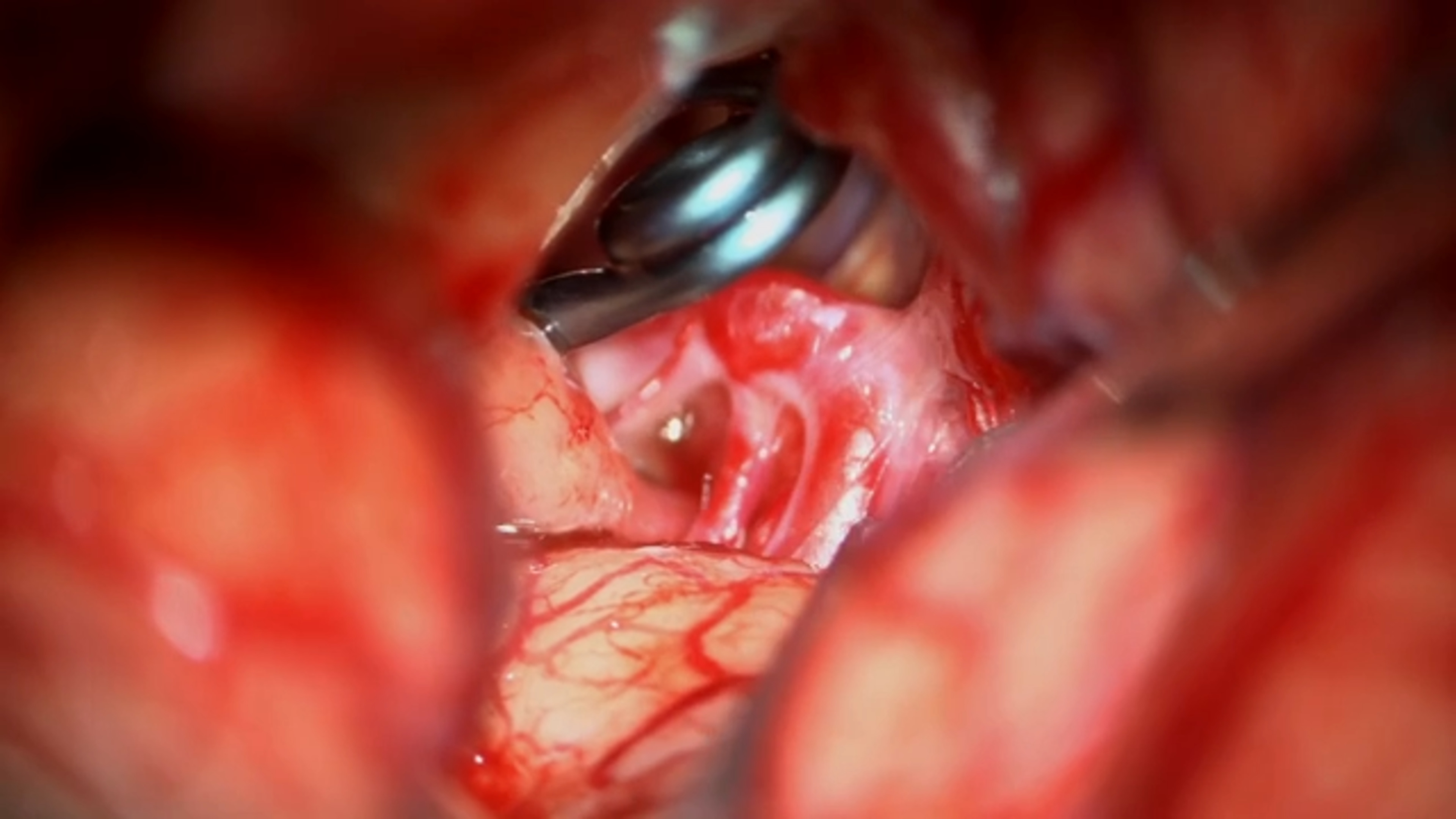
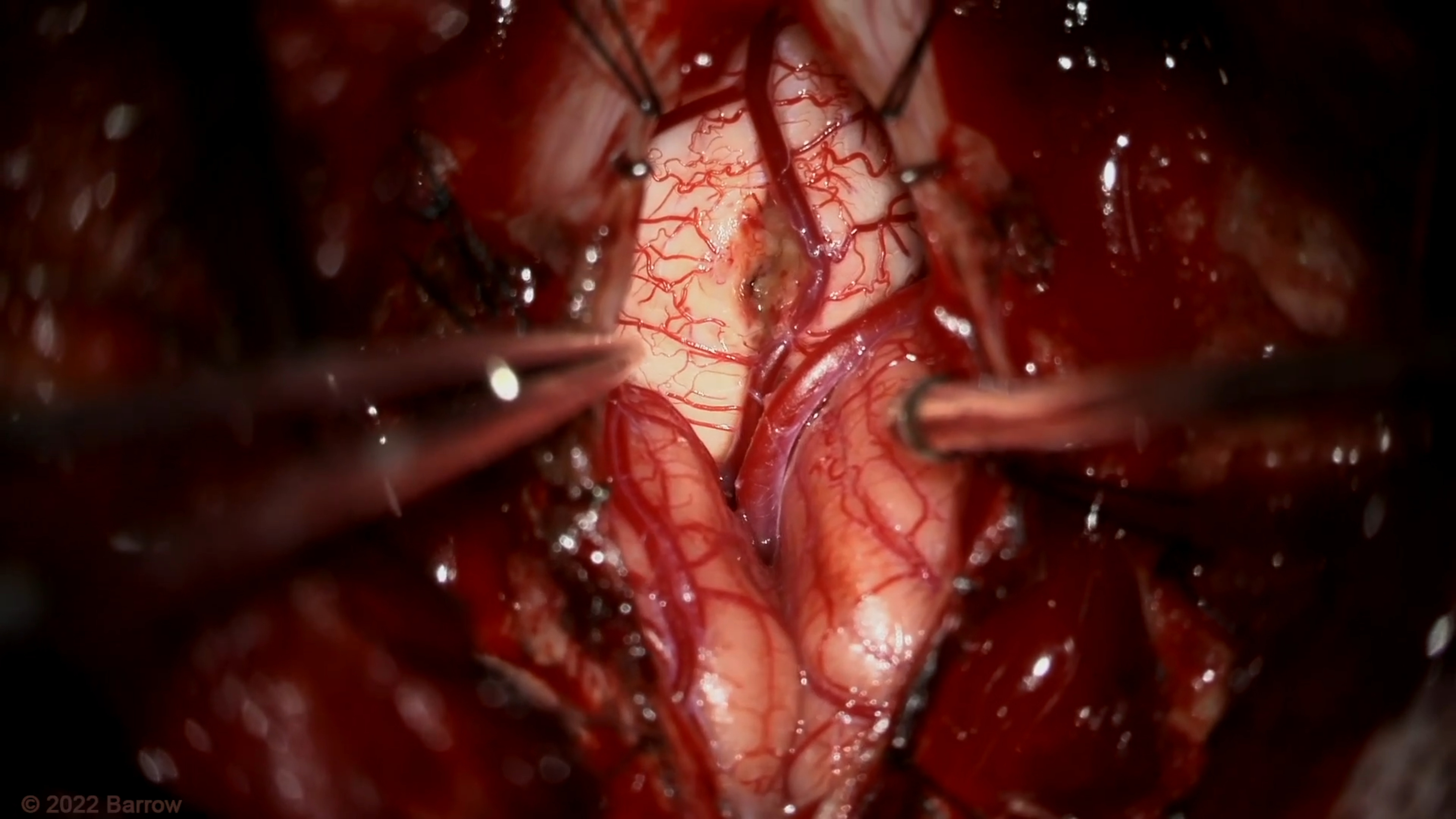
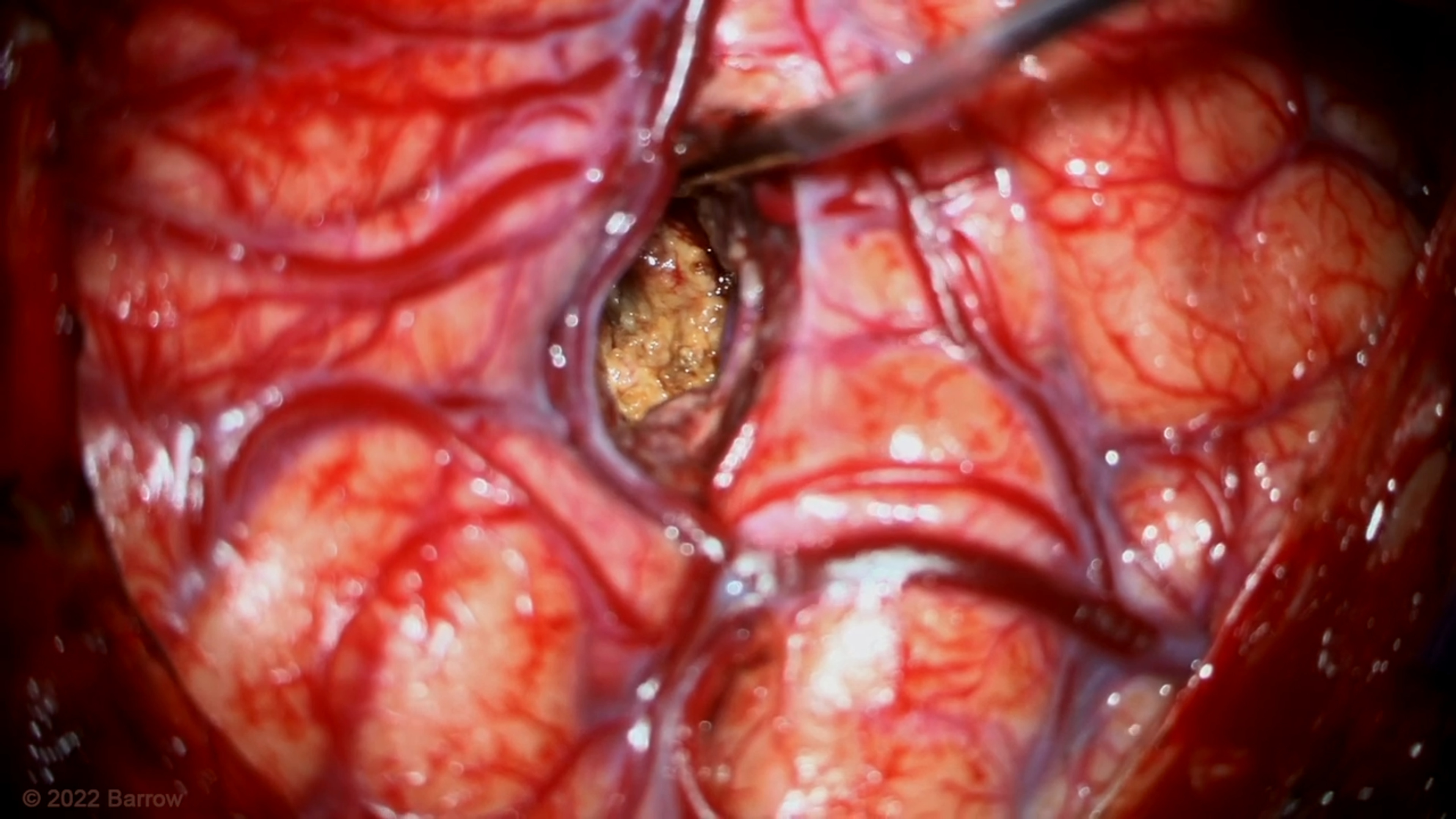
#1: Pial Resection Technique for an Eccentric Intramedullary Cervical Spinal Cord Arteriovenous Malformation
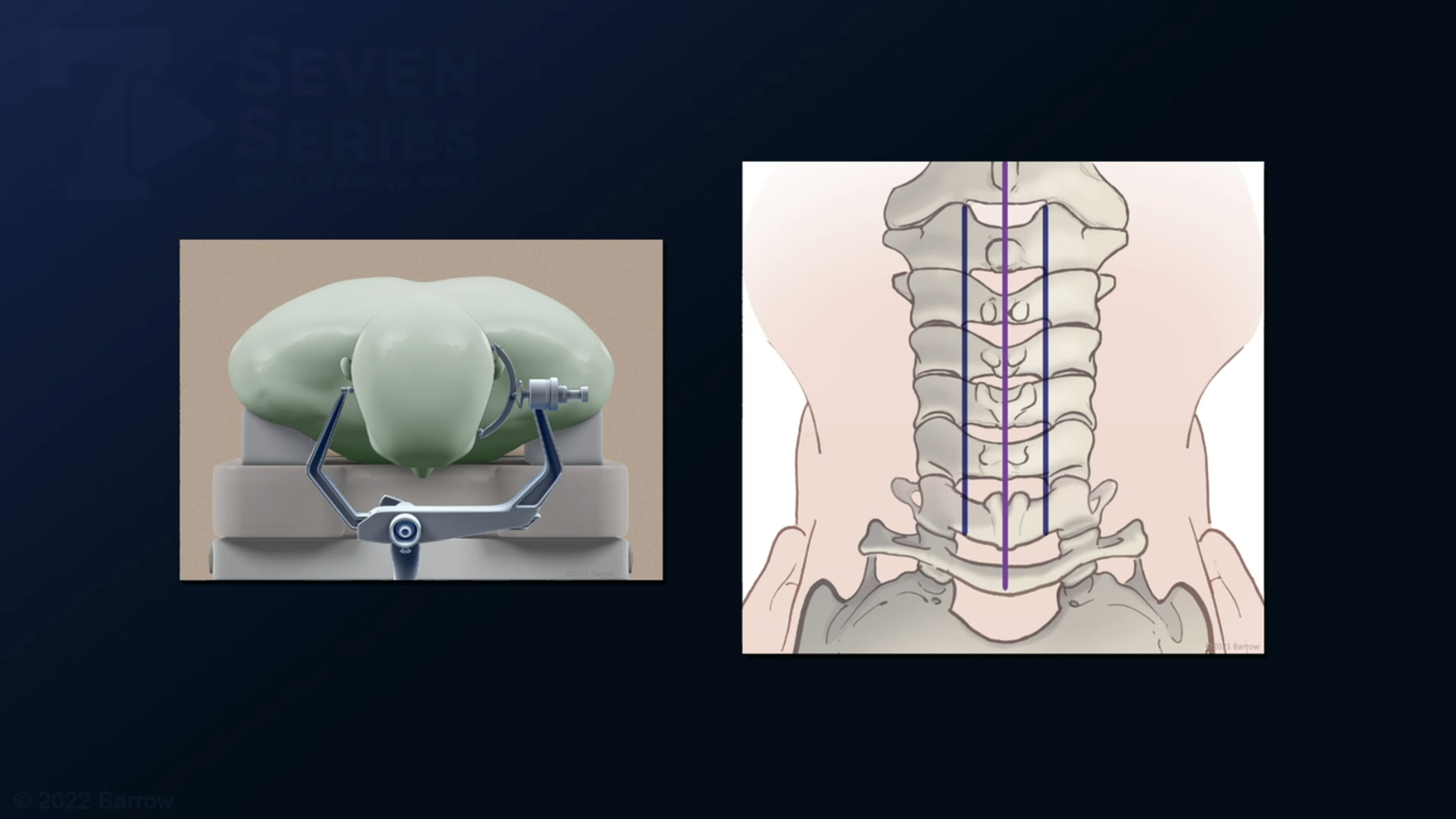
One of my favorites too, despite it being a spine case and high risk. This impressive tangle of arteries and veins engulfing the high cervical spinal cord is the “spectacular freak of nature, an explosion of hemodynamic energy and red fury” that I described in Seven AVMs. Fearsome, beautiful, almost untouchable…
Original Caption: One of the rarest and scariest lesions I treat is the intramedullary spinal AVM – one mistake and your patient may be quadriplegic. That’s why having these cases referred and getting an opportunity to treat more is so essential to advance surgical therapy. With experience, we continue to learn more about pia resection technique, nidal disassembly, venous occlusion, and surgical outcomes. To those that refer to @BarrowNeuro, thank you…