
Clinical Images: Lumbar Aneurysmal Bone Cyst Treated with Embolization, Resection, and Anterior-Posterior Fixation
Authors
A. Giancarlo Vishteh, MD
Dean G. Karahalios, MD
Cameron G. McDougall, MD
Harold L. Rekate, MD
Volker K. H. Sonntag, MD
Division of Neurological Surgery, Barrow Neurological Institute, Mercy Healthcare Arizona, Phoenix, Arizona
Key Words : aneurysmal bone cyst, bone tumor, surgical resection, endovascular
An 11-year-old girl became symptomatic with severe back pain that radiated bilaterally to her thighs. Lumbar spinal radiography (Panel A) revealed a lytic lesion involving the L1 vertebral body and pedicles. Axial computed tomography (Panel B, bone algorithm) further delineated the degree of bony destruction, which involved the L1 vertebral body, pedicles, facets, laminae, and spinous process. An axial T1-weighted lumbar magnetic resonance image (Panel C) obtained to assess spinal cord impingement showed the bony pathology and compromise of the thecal sac.
Selective spinal angiography performed before surgery showed a vascular tumor; the L1 radicular feeders were embolized with polyvinyl alcohol (Panel D). Spinal angiography performed afterward showed effective embolization of the tumor’s feeding vessels (Panel E).
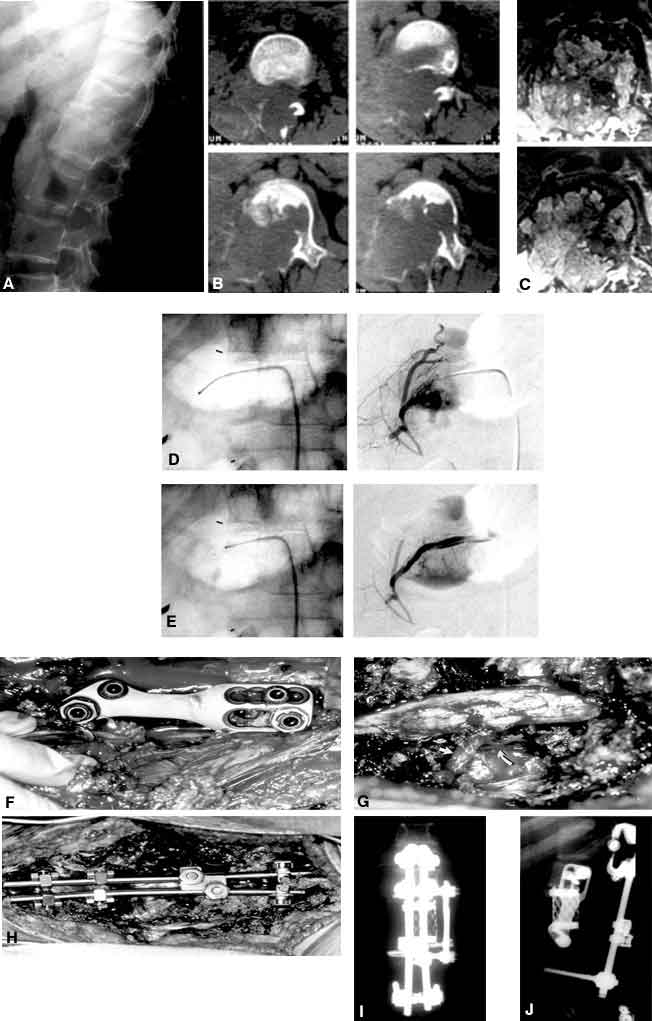
Two days later in the same operative setting, the patient underwent a combined anterior and posterior approach to her pathology. First, the L1 vertebral-body pathology was approached via a combined thoracoabdominal approach with the patient in the right lateral decubitus position. An L1 corpectomy, reconstruction with a Harm’s cage, and T12 to L2 fixation with a Z plate (Panel F) followed. The patient was repositioned prone and underwent a laminectomy with resection of the posterior aneurysmal bony elements. A view of the site of posterior decompression(Panel G) shows the L2 nerve root laterally (arrow). The Harm’s cage, which is part of the anterior construct, can be seen ventral to the thecal sac (curved arrow). Posterior fixation was accomplished with a construct that included pedicle screws, hooks and rods. The pedicle screws were placed bilaterally at L3 and the hooks were placed bilaterally at T11 (Panel H). Postoperative anteroposterior (Panel I) and lateral(Panel J) radiographs show the constructs.
Histopathological analysis was consistent with an aneurysmal bone cyst. Despite requiring superficial revision of her posterior wound, the girl was neurologically intact and without pain at her 6-month follow-up examination. Dynamic radiographs confirmed a stable fixation.