
Microsurgical Anatomy of the Clinoidal Segment of the Internal Carotid Artery, Carotid Cave, and Paraclinoid Space
Authors
Cargill H. Alleyne, Jr., MD*
Ernesto Coscarella, MD
Robert F. Spetzler, MD
Matthew T. Walker, MD
Ameet C. Patel, MD**
Robert C. Wallace, MD**
Divisions of Neurological Surgery and **Neuroradiology, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
*Current address: Department of Neurological Surgery, University of Rochester Medical Center, Rochester, New York
Abstract
Aneurysms are often encountered at the carotid siphon. The clinoidal segment of the internal carotid artery (ICA) is located at its transition from the cavernous sinus to the subarachnoid space and has been poorly understood because the anatomy of this region is complex and variable. Understanding the clinoidal segment is important for correctly diagnosing and managing these aneurysms because the risks of aneurysmal rupture vary with the specific location of lesions along this small segment of the ICA. Likewise, surgical approach depends on the exact location of the lesion. This article reviews the relationship of the ICA to the anterior clinoid process and dural rings and the risk of rupture associated with each specific type of aneurysm.
Key Words: aneurysms, anterior clinoid process, internal carotid artery
The anatomy of the small segment of the internal carotid artery (ICA) distal to its cavernous segment in the region of the anterior clinoid process, ophthalmic artery, and superior hypophyseal artery has been poorly understood.[1] Consequently, nomenclature for aneurysms arising in this region has been confusing.[5,6,8] This article briefly reviews the surgical anatomy of the clinoidal segment of the ICA, the carotid cave, and the paraclinoid space and the clinical significance of this anatomy for the growth of aneurysms in the region.
{kind=link}
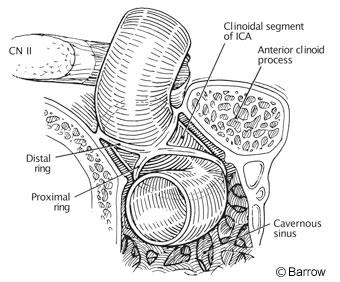
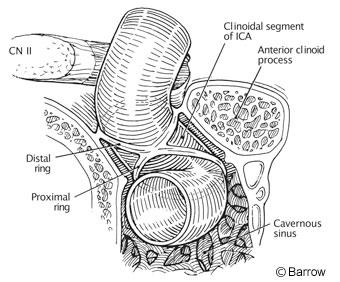
The clinoidal segment is the small transitional segment of the ICA from the cavernous sinus to the subarachnoid space (Fig. 1). The clinoidal segment is named for its relationship to the anterior clinoidal process, which is closely juxtaposed to the lateral wall of the artery. This segment is just proximal to the usual location of the ophthalmic artery, which originates from the dorsomedial wall, and to the superior hypophyseal artery, which originates from the ventromedial wall.
The anterior clinoid processes project posteromedially from the medial aspect of the lesser wing of the sphenoid. As the ICA emerges from the cavernous sinus, it is closely opposed to the inferomedial surface of the anterior clinoid process. At the anterior genu, the ICA curves anteriorly to posteriorly and also laterally to medially. Just distal to the anterior genu, it curves medially to laterally.
Two dural rings form the boundary of the clinoidal segment (Fig. 1). The proximal dural ring forms the roof of the cavernous sinus and is continuous with the dura covering the inferolateral aspect of the anterior clinoid process. The distal dural ring is another layer of dura that is continuous with the falciform ligament medially (overlying the optic nerve) and with the dura investing the superomedial aspect of the anterior clinoid process. The plane of the distal dural ring is inclined in the posteromedial direction.[8] The distal dural ring is fused with the proximal dural ring posteriorly but separated from it anteriorly to a variable degree.[1] The lateral segment of the ICA between the two rings is termed the (lateral) clinoidal segment.
{kind=link}
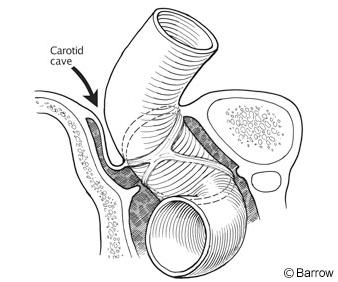
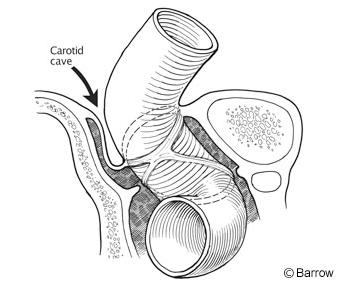
The distal dural ring firmly adheres to the adventitia of the lateral aspect of the ICA but is redundant on the medial aspect, forming the potential space of the carotid cave (Fig. 2).[5] Kobayashi et al.[5] reserve the term “clinoid space” for the lateral aspect of the ICA, which is typically considered extracavernous and extradural. In contrast, the carotid cave can contain the subarachnoid space. A recent report has slightly modified the view of the clinoidal segment,[9] suggesting that it is intracavernous. From this perspective, the clinoid segment is located within a collar formed from the dura lining the medial surface of the anterior clinoid process, the posterior surface of the optic strut, and the upper part of the carotid sulcus. The upper dural ring adheres to the wall of the artery, but the lower ring is separated from the lower margin of the clinoidal segment by a narrow space that transmits venous tributaries of the cavernous sinus.
Clinical Significance of Anatomy
Aneurysms arising from the clinoidal segment of the ICA may have a somewhat lower risk of rupturing into the subarachnoid space compared to supraclinoid ICA aneurysms. The risks of rupture associated with aneurysms arising from the medial clinoidal segment (carotid cave) and the lateral clinoidal segment (clinoidal space) also may differ. Aneurysms on the lateral clinoidal segment are extradural and extracavernous and may be relatively protected from subarachnoid rupture. Those in the carotid cave also may be partially protected but are associated with a risk of subarachnoid hemorrhage if the aneurysm extrudes through the cave.

Aneurysms in the carotid cave may arise due to the turbulence of blood flow related to its change in course at the genu of the ICA (Fig. 3A). One cadaveric dissection documented small vessels in the carotid cave coursing anteriorly to the dura of the anterior sellar region (unpublished data). Growth of carotid cave aneurysms is restricted because they are bounded by the carotid sulcus of the sphenoid bone medially and by the ICA laterally. Thus, they may be relatively protected from rupture. Continued ventromedial growth of a carotid cave aneurysm may cause it to extend into the cavernous sinus (Fig. 3B) while continued growth superiorly may cause it to extend out of the carotid cave (Fig. 3C). Characteristically, carotid cave aneurysms project medially on anteroposterior angiographic views and are either superimposed on the ICA or project posteriorly on lateral views.
Distinguishing carotid cave aneurysms from other proximal ICA aneurysms can sometimes be difficult. Ophthalmic artery aneurysms arise at the origin of the artery and usually project dorsally or dorsomedially. They tend to close the carotid siphon. Aneurysms that arise in relation to the superior hypophyseal artery can be further subdivided into paraclinoid and suprasellar.1 The paraclinoid variant projects inferiorly or inferomedially toward and beneath the anterior clinoid process and can be confused with a cavernous ICA aneurysm. This variant tends to open the siphon. The suprasellar variant is a true superior hypophyseal aneurysm and extends medially or superomedially into the suprasellar space. The paraclinoid space is delineated by the ventral ICA surface (just distal to the distal ring) superiorly, the roof of the cavernous sinus inferiorly, and the anterior petroclinoid ligament laterally. Ventral paraclinoid aneurysms6 originate from the inferior wall of the ICA opposite the origin of the ophthalmic artery and project inferiorly, or inferiorly and slightly medially. They frequently grow toward the cavernous sinus. Their growth is limited laterally by the petroclinoid ligament.
Conclusion
A small segment of the ICA between the cavernous sinus and ophthalmic artery is of enormous clinical importance. Although definitions and classification systems abound, categorizing an individual aneurysm in this region can be difficult. It may be impossible to predict the exact site of the origin of some aneurysms arising in this region because of their size and the complexity of the dural, bony, and arterial relationships of the region. Surgical treatment of aneurysms arising in this region is technically challenging and extensively described elsewhere.[1-5,7,10] Appreciation of the anatomic relationships of this area, however, will improve the diagnosis and treatment of associated lesions.
References
- Day AL: Aneurysms of the ophthalmic segment. A clinical and anatomical analysis. J Neurosurg 72:677-691, 1990
- Fox JL: Microsurgical treatment of ventral (paraclinoid) internal carotid artery aneurysms. Neurosurgery 22:32-39, 1988
- Heros RC, Nelson PB, Ojemann RG, et al: Large and giant paraclinoid aneurysms: Surgical techniques, complications, and results. Neurosurgery 12:153-163, 1983
- Knosp E, Müller G, Perneczky A: The paraclinoid carotid artery: Anatomical aspects of a microneurosurgical approach. Neurosurgery 22:896-901, 1988
- Kobayashi S, Kyoshima K, Gibo H, et al: Carotid cave aneurysms of the internal carotid artery. J Neurosurg 70:216-221, 1989
- Nutik S: Carotid paraclinoid aneurysms with intradural origin and intracavernous location. J Neurosurg 48:526-533, 1978
- Nutik SL: Removal of the anterior clinoid process for exposure of the proximal intracranial carotid artery. J Neurosurg 69:529-534, 1988
- Oikawa S, Kyoshima K, Kobayashi S: Surgical anatomy of the juxta-dural ring area. J Neurosurg 89:250-254, 1998
- Seoane E, Rhoton AL, Jr., de Oliveira E: Microsurgical anatomy of the dural collar (carotid collar) and rings around the clinoid segment of the internal carotid artery. Neurosurgery 42:869-886, 1998
- Yasargil MG, Gasser JC, Hodosh RM, et al: Carotid-ophthalmic aneurysms: Direct microsurgical approach. Surg Neurol 8:155-165, 1977