
Hyperprolactinemia
At a Glance
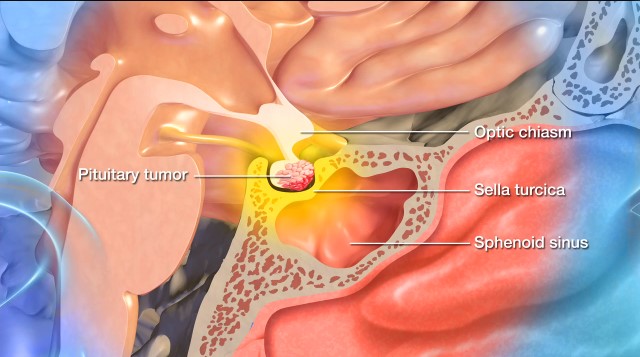
- Hyperprolactinemia involves abnormally high prolactin levels, most often caused by a benign pituitary tumor (prolactinoma).
- Symptoms in women include irregular periods, milky breast discharge, and low estrogen. Men may experience low libido, erectile issues, or breast enlargement.
- Diagnosis involves a blood test for prolactin levels and medical imaging to check for a pituitary tumor.
- Treatment usually starts with medication to lower prolactin and shrink the tumor. Surgery or radiation may be used if medications are ineffective.
Overview
Hyperprolactinemia describes abnormally high levels of the hormone prolactin. In some people, it doesn’t cause symptoms. In contrast, in others, it can cause galactorrhea, or milky discharge from the breasts not related to pregnancy or breastfeeding, and oligomenorrhea and amenorrhea, which is irregular or absence of menstrual periods in a woman of reproductive age.
The degree to which prolactin levels are elevated is an important factor. Most often, the underlying cause of excess prolactin levels is a prolactinoma, a benign or noncancerous tumor of the pituitary gland that secretes too much prolactin.
Excessive levels of prolactin can lead to the cessation of menstrual cycles resulting in decreased fertility and estrogen levels that cause additional symptoms, like hot flashes, skin and vaginal dryness, mood changes, headaches, fatigue, trouble concentrating, and ultimately, bone loss.
What causes hyperprolactinemia?
The underlying cause of these excess prolactin levels is frequently a prolactinoma.
Other potential causes of hyperprolactinemia include the following:
- Pituitary stalk compression: A tumor or mass that presses on the pituitary stalk can reduce dopamine inhibition, which increases prolactin levels. Dopamine acts as the primary inhibitor of prolactin secretion, meaning that high dopamine levels suppress prolactin production. Conversely, when dopamine levels are low, prolactin production increases.
- Hypothalamic tumors: Abnormal growths on the hypothalamus gland—such as craniopharyngiomas, germinomas, and hypothalamic hamartomas—can disrupt dopamine signaling, which inhibits prolactin secretion.
- Medications: Certain medications can block dopamine’s ability to inhibit prolactin, including:
- Antipsychotics like risperidone or haloperidol
- Antidepressants like selective serotonin reuptake inhibitors (SSRIs) or tricyclics
- Opioids
- Antihypertensives used to lower blood pressure.
- Hypothyroidism: Also known as low thyroid hormone levels, this condition can cause increased thyrotropin-releasing hormone and thyrotropin stimulation hormone, which stimulates prolactin release.
- Polycystic ovary syndrome (PCOS): This hormonal disorder that occurs during the reproductive years of women can cause irregular menstrual cycles and can cause mild cases of hyperprolactinemia.
- Infiltrative diseases: Diseases like sarcoidosis or tuberculosis can also affect the hypothalamus, affecting prolactin secretion.
Other causes include chronic stress and excessive exercise, which can temporarily elevate prolactin levels. Chronic kidney disease or liver disease can also impair the clearance of prolactin from the blood, leading to excess prolactin.

Symptoms of Hyperprolactinemia
The symptoms of hyperprolactinemia are the direct result of high prolactin levels and, consequently, the disruption of normal reproductive hormone function.
Beyond the primary symptoms of galactorrhea—abnormal milk production in women who are not pregnant or breastfeeding—and amenorrhea—the absence of menstrual periods for three or more months—you or someone you know might experience a combination of the following symptoms:
- Galactorrhea: This atypical milk production in women who aren’t pregnant or breastfeeding can look like sporadic or consistent milky discharge from one or both of your nipples and can occur on its own or when your breast is touched. This is not a reason to think that you have breast cancer.
- Amenorrhea: Hyperprolactinemia can result in missing your menstrual periods for three months or more.
- Decreased fertility: As a result of suppressed ovulation and amenorrhea, infertility can occur.
- Low estrogen symptoms: Hyperprolactinemia can cause low estrogen levels, similar to the state of menopause, resulting in hot flashes, mood swings, low energy, low sex drive, weight gain, night sweats, lowered libido, and vaginal dryness.
- Headaches: Headaches can occur with pituitary tumors and low estrogen levels caused by high prolactin levels. Pituitary tumor headaches are typically located on the forehead or behind the eyes but can vary in location and intensity. Meanwhile, a hormonal headache or migraine can feel like a throbbing pain on one side of your head.
- Vision problems: Pituitary tumors can press on the optic nerve, causing vision problems like the loss of your peripheral vision or double vision.
- Bone loss: Due to prolonged estrogen deficiency, osteopenia or osteoporosis can develop. Osteopenia is a precursor to osteoporosis, which weakens bones and makes them more susceptible to fractures. Osteoporosis is a disease that weakens bones, causing the body to lose bone mass faster than it can rebuild.
Symptoms like a severe headache, dramatic changes to vision, and sudden hormonal deficiencies should prompt an immediate medical evaluation. These can be symptoms of pituitary apoplexy or sudden tumor bleeding in the case of a pituitary tumor, a rare condition associated with the presence of pituitary tumors, including prolactinomas. Early detection and treatment can help prevent complications and improve outcomes.
Diagnosis of Hyperprolactinemia
Blood tests measuring prolactin levels, along with imaging studies to help visualize any potential pituitary tumors, are usually the tests performed to confirm the diagnosis.
Doctors use the following exams and imaging tests to perform a diagnostic workup:
- Physical exam: First, your healthcare provider will ask about your symptoms, overall health, medication history, and family history. Next, they’ll perform a physical exam to assess the cause of menstrual irregularities and galactorrhea and check for any vision changes.
- Magnetic Resonance Imaging (MRI): Imaging studies are crucial in visualizing organs and identifying abnormalities, and an MRI is a gold standard for detecting pituitary tumors, like prolactinomas, or other pituitary abnormalities. An MRI will provide detailed images of the pituitary gland and its surrounding structures. Your doctor may refer you for a brain MRI if other hypothalamic or pituitary lesions are suspected.
- Computed Tomography (CT): CT scans are used when an MRI is not feasible, for example if you have a pacemaker, or if additional evaluation of the surrounding structures is needed. CT scans rely on X-rays to create detailed cross-sectional images of the brain or other organs.
- Hormonal testing: Key hormonal tests to diagnose hyperprolactinemia can include:
- Serum prolactin levels test: Elevated prolactin levels will confirm hyperprolactinemia and potentially suggest a prolactinoma if they are high enough.
- Thyroid function test: This test analyzes certain thyroid hormones, like TSH and Free T4, to rule out hypothyroidism, which can lead to high prolactin.
- Gonadotropin levels and estradiol test: These tests assess reproductive hormone suppression. Low luteinizing and follicle-stimulating hormones indicate suppressed ovarian function due to high prolactin, while low estradiol confirms an estrogen deficiency, which can lead to amenorrhea and the risk of bone loss.
- Pregnancy test: Importantly, your doctor will need to rule out pregnancy needs, as it is a cause of high prolactin and amenorrhea.
You may also be referred to an eye doctor for a vision test since pituitary tumors can damage optic nerves and cause vision problems. In rare cases, further hormone stimulation testing may be done to assess pituitary function.
Your doctor can use the information from these tests to confirm a diagnosis and work with you to decide on a treatment plan.

Treatments for Hyperprolactinemia
Treatment will depend on the underlying cause, but often involves the following nonsurgical treatments—primarily dopamine agonists like cabergoline or bromocriptine.
Nonsurgical Treatments
- Dopamine agonists: As a first-line treatment, dopamine agonists are medications that lower prolactin levels, shrink prolactinomas, restore ovulation, and stop galactorrhea in most cases. Examples include cabergoline, which physicians prefer due to higher efficacy and fewer side effects, and bromocriptine, which is an alternative that’s often used for pregnancy planning. Dopamine agonists help restore prolactin levels to normal in more than 90% of amenorrhea-galactorrhea syndrome cases.
- Treating underlying conditions: Hypothyroidism can be treated with the medication levothyroxine, which can lower prolactin levels, while medication-induced hyperproteinemia can be addressed by adjusting or stopping the responsible drug if advised. Polycystic ovary syndrome (PCOS) can also be treated with hormonal therapy, such as birth control pills.
- Estrogen replacement therapy: Should estrogen levels remain low and ovulation doesn’t return, your doctor might prescribe birth control pills or estrogen-progesterone therapy. These medications can help prevent bone loss and cardiovascular risks due to long-term estrogen deficiency.
- Lifestyle modifications: High cortisol, a byproduct of high stress, can contribute to hormonal imbalances and lead to elevated prolactin levels. Excessive exercise can also temporarily elevate prolactin levels.
Some cases of hyperprolactinemia are caused by a nonfunctioning tumor, which can raise prolactin levels. However, prolactin levels stemming from a nonfunctioning tumor tend to be lower than those caused by prolactinomas. Dopamine agonists can lower prolactin levels caused by a nonfunctioning tumor, but unlike a prolactinoma, the tumor will not shrink in response. In some complex cases, surgery or radiation therapy may be needed if the tumor is resistant and does not respond to dopamine agonists or continues to grow despite dopamine agonist treatment.
Surgical Treatments
If dopamine agonists are not well-tolerated or don’t work, or when a tumor is large and putting pressure on nearby structures, your team may recommend surgery. The procedure will depend on the tumor’s size, type, location, and impact on surrounding tissues.
- The most common surgical approach for a pituitary tumor is transsphenoidal surgery. This is when a neurosurgeon reaches and removes the tumor through the nasal passages and the sphenoid sinus using a small surgical instrument and an endoscope.
Finally, in rare cases, radiation therapy can be used if a prolactinoma is not responding to medication or surgery, or continues to grow. Radiation therapy uses precisely aimed beams of radiation to destroy tumors in the body. While it doesn’t remove the tumor, it damages the DNA of the tumor cells, which lose their ability to reproduce and eventually die. However, its tumor-shrinking effects may take months or even years to develop.
Common Questions
How common is hyperprolactinemia?
Hyperprolactinemia affects around 0.4% of the general population. It can affect upwards of 5% of women who have reproductive disorders like endometriosis or PCOS.
Prolactinomas are the most common cause of hyperprolactinemia, occurring in 3 to 5 out of every 100,000 people each year. They are more frequent in women of reproductive age. Another frequent trigger of hyperprolactinemia can be medication-induced hyperprolactinemia, which can happen in any person taking antipsychotics, antidepressants, or dopamine-blocking drugs.
Who gets hyperprolactinemia?
The most commonly affected groups include:
- Women of reproductive age: Women between 20 and 40 years old are most frequently affected, as prolactin imbalances disrupt the menstrual cycle and ovulation. Women tend to present earlier because of these symptoms. In contrast, men may only develop symptoms of low testosterone and low sex drive. Generally, men are less likely to seek medical attention for such symptoms.
- Individuals taking certain medications: These medications can include antipsychotics, antidepressants, opioids, antihypertensives, and some hormonal medications precisely because they interfere with the regulation of prolactin by blocking dopamine receptors in the brain. This, in turn, leads to elevated prolactin levels. Medication-induced hyperprolactinemia can happen to anyone at any age, although it’s most common in women between 20 and 35 years old.
- People with pituitary or hypothalamic disorders: Prolactin-secreting tumors like prolactinomas or hypothalamic lesions can disrupt hormonal regulation, leading to amenorrhea-galactorrhea syndrome.
- People with endocrine disorders: Hypothyroidism can cause excess stimulation of prolactin, while polycystic ovary syndrome (PCOS) can be associated with mild hyperprolactinemia.
- Men: Although men cannot experience amenorrhea, men can experience a similar syndrome called male hypogonadism, which causes galactorrhea, low testosterone, erectile dysfunction, and infertility. However, these cases are often linked to larger pituitary tumors known as macroprolactinomas.
What is the prognosis?
The prognosis is usually favorable. Most people respond well to treatment and regain their normal quality of life, though this depends on the underlying cause of the excess prolactin.
If a prolactinoma causes hyperprolactinemia, medication or surgery will often reduce tumor size, normalize prolactin levels, and relieve symptoms. In medication-induced hyperprolactinemia, stopping or switching medications will usually resolve the symptoms in a matter of weeks. In the event of hypothyroidism, treatment with levothyroxine can restore prolactin balance and regular menstrual cycles.
Can amenorrhea and galactorrhea be prevented?
No is the short answer, especially when the condition is caused by genetic factors, pituitary tumors, or underlying endocrine disorders. However, specific strategies can help reduce your risk, including:
- Managing medications: If you’re taking antipsychotics, antidepressants, or dopamine-blocking drugs, you can discuss medication alternatives with your healthcare provider.
- Tending to underlying health conditions: Hormonal disorders like hypothyroidism need to be treated promptly to prevent high levels of prolactin stimulation. So, too, should polycystic ovary syndrome (PCOS), which can contribute to mild hyperprolactinemia.
If you have irregular periods or unexplained lactation, it’s essential to seek medical evaluation early. Regular check-ups can help detect pituitary disorders before your symptoms worsen.


