
Migraine
Overview
Migraine is a neurologic disease (or brain disease) in which the brain’s sensory pathways for pain activate spontaneously, leading to headache attacks and symptoms such as nausea, light sensitivity, and sound sensitivity. Attacks can last from hours to days and vary in severity. Pain from migraine attacks is also variable, but classically is described as moderate to severe throbbing on one side of the head.
Migraine can be categorized based on headache frequency:
- Episodic migraine: Headaches occur on 14 or fewer days in a month.
- Chronic migraine: Headaches occur on 15 or more days of the month, with at least eight days presenting as a headache consistent with a migraine attack.

Causes of Migraine
Migraine is a problem where the pain pathways in the brain have a genetic tendency to activate in the presence of certain environmental conditions called triggers. Identifying migraine triggers can be difficult, because something that appears to trigger a headache can actually be irritating or a feature of a headache that has already begun.
In people with migraine, the brain processes pain and sensory signals abnormally. During an attack, pain pathways in the brain and surrounding nerves become overactive, and changes in brain chemicals and blood vessel signaling amplify these signals. The result is a migraine attack that can cause symptoms like head pain along with nausea, light and sound sensitivity, and sometimes aura.
One of the key chemicals involved in migraine is calcitonin gene-related peptide, or CGRP. This compound is a signaling molecule released by nerves during a migraine attack that increases pain signaling and sensitivity in the brain. Many newer migraine treatments work by blocking CGRP or its effects, helping calm these overactive pain pathways and reduce migraine attacks.
Migraine Symptoms
There are four different symptom phases of migraine.
Phase I – Prodrome
Prodrome, or the premonitory phase, can occur hours or days before you have a migraine attack. You may notice symptoms such as specific food cravings, unexplained mood changes, uncontrollable yawning, light or noise sensitivity, increased thirst and urination, fluid retention, and neck stiffness. Sometimes, people mistake prodrome symptoms for migraine triggers. For example, if one of your prodromal symptoms is light sensitivity, you may think a certain light is a migraine trigger when it really isn’t.
Recognizing signs of the prodrome phase, if present, can be helpful for early treatment of the attack.
Phase II – Aura
Aura can occur before the headache, during the headache, or even without a headache. The duration of aura can vary, but it generally lasts between five minutes and one hour. Aura occurs in 30% of people with migraine.
The most common types of aura are:
- Visual: Visual aura can include flashing lights, zigzag lines, blind spots, or blurred spots. These changes often start small, spread across the visual field, and can be colorful.
- Sensory: Sensory aura describes unusual sensations like tingling or numbness, typically on one side of the body. It often starts in the hand or face but can spread along that side of the body over minutes. Sensory aura can also cause a feeling of heaviness in your limbs that you might mistake for the weakness of hemiplegic migraine (temporary weakness or paralysis on one side of the body).
- Language: It is not uncommon to experience brain fog that creates some word-finding difficulties during a migraine attack. However, with a language aura, there is a clear start and finish with difficulty speaking and/or understanding speech that lasts from 5-60 minutes.
Some people experience more than one type of aura at the same time, often in a predictable sequence.
Rare types of aura include hemiplegic migraine, brainstem aura (vertigo, speech difficulty or slurring, ringing in the ears, and vision problems), and retinal migraine (vision loss or visual disturbances in one eye).
Aura can be frightening, especially the first time it happens. However, it causes no lasting harm.
Migraine Aura versus Stroke
Aura symptoms can be confused with those of a stroke. The chart below explains some key differences between migraine aura and stroke.
Better safe than sorry: You should call 9-1-1 right away if you think you are having a stroke. A stroke is a life-threatening emergency, and time is of the essence.
| Symptom or Feature | Migraine Aura | Stroke |
|---|---|---|
| Onset | Gradual; builds over 5–20 minutes. | Sudden; happens instantly or in seconds. |
| Duration | Usually lasts 5–60 minutes. | Can be permanent or last hours (TIA lasts minutes). |
| Spreading | Symptoms spread slowly across the body or vision. | Multiple symptoms usually appear all at once. |
| Face / Arms | Weakness is rare (except in hemiplegic migraine). | Facial drooping and arm weakness are hallmark signs. |
| Headache | Often follows or accompanies aura; typically throbbing on one side. | Headache is rare and not consistent with migraine, or it is sudden and intense. |
Phase III – Headache
During the headache phase of a migraine, a number of symptoms are experienced that build over time, lasting hours to days. These include:
- Pain: Often described as pulsating or throbbing, migraine head pain can also feel like pressure or aching. It is often worse on one side of the head.
- Sensitivity to light, sounds, or smell is also common.
- Your head may be tender to the touch.
- Nausea with or without vomiting is common.
- You may feel tired or experience brain fog.
Phase IV: Postdrome
In the postdrome phase, exhaustion, moodiness, dizziness, and light or sound sensitivity can continue for hours or days.

Migraine Diagnosis
Since there is no specific test to confirm migraine, a diagnosis is primarily based on a description of your headaches, your medical history, a physical examination, and ruling out any other potential causes or similar conditions. Your physician will use diagnostic criteria from the International Classification of Headache Disorders (ICHD).
Your doctor might use the following exams, tests, and imaging to diagnose migraine:
- History: First, your provider will ask about your symptoms, when they began, how they’ve progressed or changed over time, and how often your attacks occur. They will also want to know what treatments you’ve tried and how well they have worked for you. They may ask about associated diagnoses as well as your family history of migraine. These questions will help your provider confirm if you meet criteria for migraine or another disorder, as well as identify the best next steps in management.
- Physical and neurological exam: Next, your provider will assess your neurological function, including your eyes, reflexes, coordination, strength, and sensation. They will often assess how well you can move your neck or ask about muscle spasms.
- Blood tests: While doctors don’t typically use these to diagnose migraine, blood tests can help rule out other conditions that may trigger migraine or cause other types of headaches.
- Magnetic Resonance Imaging (MRI) or Computed Tomography (CT) Scan: These imaging studies are crucial for visualizing the brain and identifying abnormalities if there are concerning findings during your assessment. However, imaging the brain will not aid in the diagnosis of migraine or change how you manage it. Most people with migraine do not need an MRI or CT of the brain.
If you’re concerned about any new or recurring symptoms, it’s important to speak with your healthcare provider. Not only will they provide a diagnosis for you, but they can also start a treatment plan and refer you to a headache specialist or a neurologist if needed.

Migraine Treatments
At this time, there is no cure for migraine. Still, numerous medications and therapies can help manage your symptoms when they happen, and you can take steps to reduce the frequency and severity of your migraine episodes.
Two broad classes of migraine treatments are acute (also called rescue or abortive treatments) and preventative (also called prophylactic). Acute treatments stop or lessen the severity of a migraine attack that is in progress. In contrast, preventative treatments are taken on a regular schedule and aim to reduce the frequency or severity of attacks.
Acute Treatments
Acute treatments are given when a migraine attack has already started. All patients with migraine should have rescue treatment ready to be used at the start of the headache to prevent the attack from continuing. The longer you wait to treat a migraine attack, the less likely it is to respond to acute treatments.
Triptans
Triptans provide fast relief by acting on receptors in your brain that impact the neurotransmitter serotonin and are involved in migraine signaling. These medications work by reducing the release of pain-related chemicals like CGRP, thereby decreasing the transmission of pain signals in the brain.
Triptan medications are available as tablets that you swallow, tablets designed to dissolve in your mouth, nasal sprays, and subcutaneous (under the skin) injections. You should not use triptans if you have a history of vascular disease like stroke or heart attack. Triptan sensations, a common side effect, can feel like a tightness in the chest or throat. These sensations might be uncomfortable, but they are not dangerous.
Dihydroergotamine (DHE)
Migraine specialists prescribe dihydroergotamine (DHE) as an injection or nasal spray. DHE binds to multiple signaling systems involved in migraine, such as serotonin, dopamine, and adrenergic receptors, stopping overactive migraine circuits and reducing the release of pain-related chemicals. Unlike many other acute treatments, DHE sometimes works even late in an attack.
You shouldn’t use DHE if you have a history of vascular disease, like stroke or heart attack, or within 24 hours of taking a triptan. Nausea is common with injectable forms of DHE, so your care team will likely provide you with a medication to reduce nausea and vomiting to take beforehand.
Acute Gepants
Gepants are a newer class of medications that block the activity of CGRP. They can be used both as acute and preventative treatments. Gepants are safe for people who can’t take triptans or DHE because of vascular diseases.
Gepants are generally well-tolerated; however, CGRP medications have been associated with worsening of Raynaud’s syndrome, and rarely, an increase in blood pressure. There are three gepants available for the acute treatment of migraine:
- Ubrelvy (ubrogepant) is a pill that you can take again after two hours if the first dose is fully ineffective.
- Nurtec ODT (rimegepant) is an orally dissolving tablet that you can take once every 24 hours.
- Zavzpret (zavegepant) is a nasal spray that you can use once every 24 hours.
Over-the-counter (OTC) Medications
Many people with migraine try over-the-counter medications before seeing a physician. Non-steroidal anti-inflammatory drugs (NSAIDs) like Advil (ibuprofen) and Aleve (naproxen) are two of the most commonly used OTC options, as well as medications that mix NSAIDs with caffeine, like Excedrin. Both prescription and OTC NSAIDs can be effective acute treatments for migraine attacks, as can Tylenol (acetaminophen).

Preventative Treatments
Preventative treatments are medications in the form of pills and injections that are taken consistently over time to reduce the frequency and severity of migraine. As an added benefit, they can also increase the effectiveness of rescue treatments.
Doctors often recommend preventative treatment for patients who have approximately four or more headache days per month. These treatments can start working to reduce headaches within a week, but the maximum benefit might take a few months or more to notice.
Botox
Botox (botulinum neurotoxin, also called onabotulinumtoxinA) is an effective treatment for chronic migraine. Researchers think it works by preventing the release of CGRP. Botox treatment for migraine consists of 31 or more injections in the head and neck, administered every 12 weeks. Some people see improvement in the first month, but it can take 2-3 injection appointments to see maximum benefit.
CGRP Monoclonal Antibodies
Monoclonal antibodies that block CGRP can be administered as once-monthly or every 3 months injections at home or by IV infusion once every three months. The subcutaneous injections can cause an injection site reaction (pain, redness, swelling), while IV infusion can cause an infusion reaction with flu-like symptoms.
- Aimovig (erenumab): This monthly injection comes as a 70mg or 140mg subcutaneous injection.
- Ajovy (fremanezumab): This subcutaneous injection can either be administered as 225mg every month or as 675mg every 3 months.
- Emgality (galcanezumab): This monthly injection comes as a 120mg subcutaneous injection, but the first month is injected as a 240mg loading dose.
- Vyepti (eptinezumab): This medication is an infusion given through an IV at an outpatient infusion center every 3 months. It comes in 100mg and 300mg doses.
Preventive Gepants
Like the acute version, preventative gepants block CGRP and are generally well tolerated. The two gepants approved for preventative use are:
- Nurtec (rimegepant): A tablet that dissolves in your mouth, which is taken every other day
- Qulipta (atogepant): A pill that is available in several dosages and is taken daily.
Note: CGRP medications, including CGRP monoclonal antibodies and gepants, can cause nausea, worsening of Raynaud’s, and rarely an increase in blood pressure for some people. These side effects are less common with acute use of gepants.
Nonspecific Preventive Medications
Many older medications originally made for another purpose can help with migraine as well. These include:
- Blood pressure medications: Beta-blockers (e.g., propranolol or metoprolol), candesartan, and lisinopril may help reduce the frequency and severity of migraine, even if you do not have hypertension.
- Antidepressants: This class of medications can be effective in preventing migraine—even in those without depression—and include tricyclic antidepressants (for example, amitriptyline) and serotonin-norepinephrine reuptake inhibitors (for example, venlafaxine).
- Antiseizure medications: Antiseizure medications like topiramate and valproate/divalproex may also reduce the frequency of migraine attacks even in people without epilepsy or seizures.
Other Migraine Treatment Options
Nerve Blocks and Trigger Point Injections
Nerve blocks and trigger point injections are used both as preventative and acute therapies. Migraine specialists also prescribe them as a transitional treatment for some patients, using them to eliminate extreme or prolonged migraine attacks while preventative treatments start working.
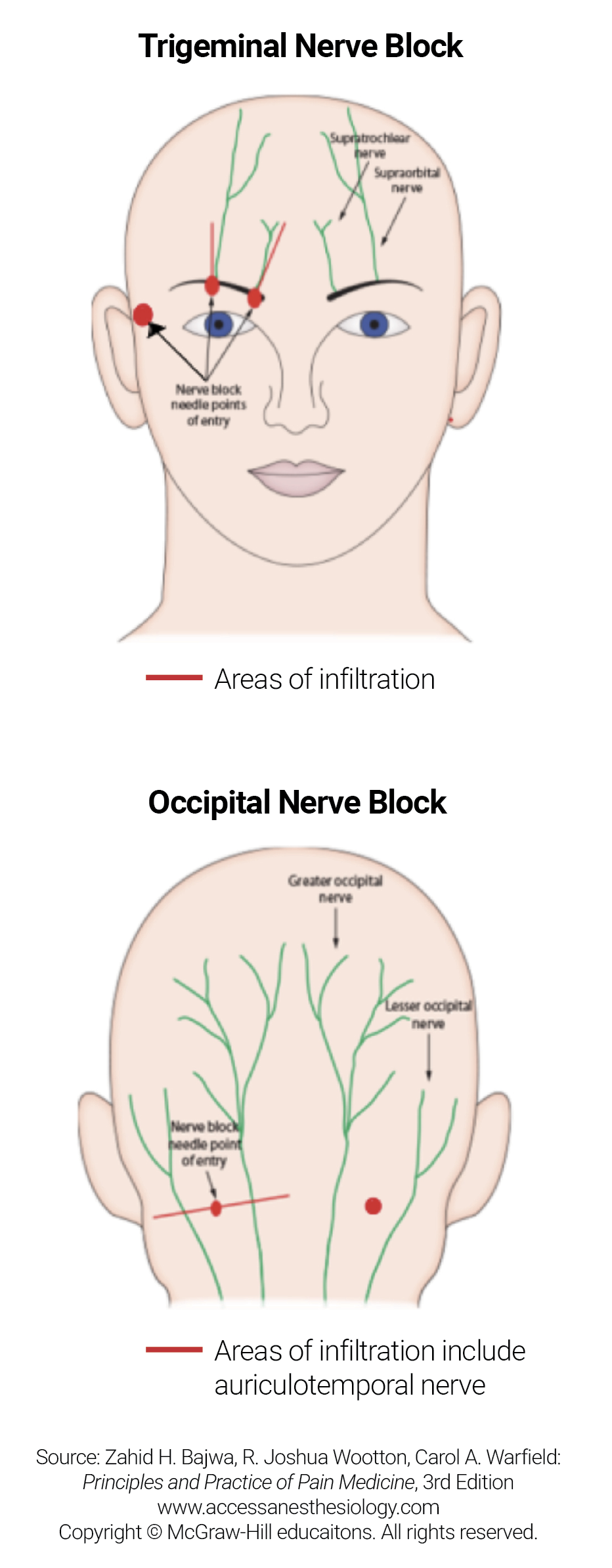
Trigeminal and Occipital Nerve Blocks
These nerve blocks involve injecting a local anesthetic (for example, ropivacaine, bupivacaine, or lidocaine) into the area around branches of the trigeminal or occipital nerve, which connect the front and back of the head to the brain, respectively. People often notice improvement soon after treatment, and the vast majority tolerate the injections well.
Sphenopalatine Ganglion (SPG) Blocks
The sphenopalatine ganglion (SPG) is a small bundle of nerves located deep behind the nose that functions as a relay station for pain signals. During an SPG block, your provider will advance a flexible catheter up the nostril toward the SPG, then slowly drip lidocaine onto the nerve endings.
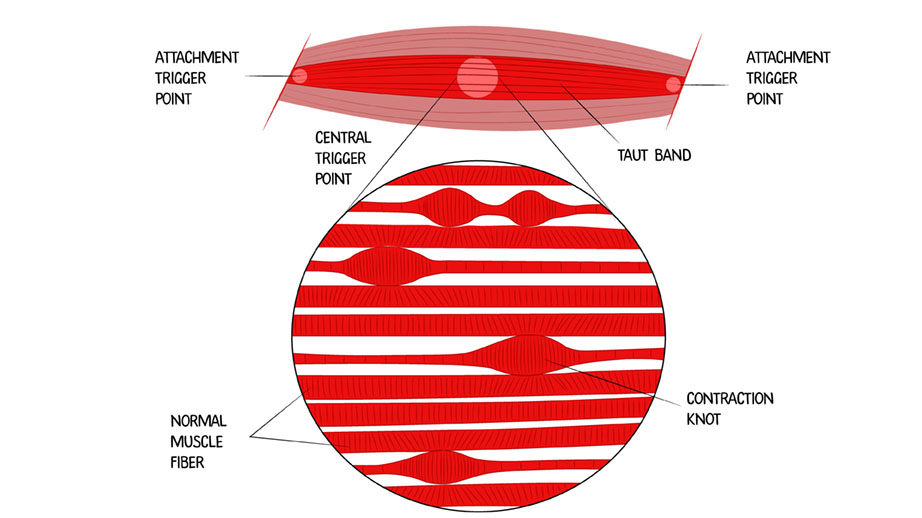
Trigger Point Injections (TPIs)
Trigger point injections (TPIs) differ from nerve blocks because, rather than focusing on groups of nerves, they target muscles in the shoulder and neck to relieve migraine attacks caused by muscle tightness. Migraine specialists also use local anesthetics in these injections, often combining them with nerve blocks.
Devices and Neuromodulation
Neuromodulation is the use of devices that emit electrical or magnetic fields to treat migraine. Some types of neuromodulation work to prevent migraine attacks, while others work to treat an attack once it occurs

Behavioral Treatments
In addition to medication, mindfulness, cognitive behavioral therapy (CBT), biofeedback, acupuncture, and yoga are all well-studied approaches for the management of migraine and associated symptoms. These treatments can be beneficial for anyone with migraine, even if you don’t have a mood disorder like depression or anxiety.
Migraine can lead to debilitating stress, grief for the loss of your previous lifestyle, and frustration. All of these reactions are normal and common, but they can worsen your quality of life. Even if you feel your coping skills are adequate, behavioral treatments can help you better manage your symptoms.
As such, migraine often benefits from a multidisciplinary approach that includes behavioral techniques like these:
- Cognitive behavioral therapy (CBT) trains your brain’s alarm system not to overreact to triggers (both physical and emotional), which migraine makes the brain more prone to doing.
- Mindfulness, which involves concentrating on the present moment, functions like a volume knob for your brain. Migraines cause the brain to react excessively to stimuli in the environment. By practicing mindfulness, you can reduce the background noise around you, helping to prevent your brain from becoming overloaded with information that may trigger a migraine attack.
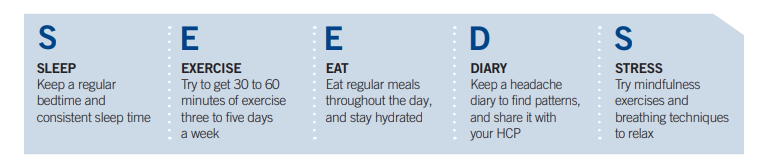
Lifestyle Management
Simple but consistent changes to your lifestyle— maintaining good sleep habits, staying hydrated, eating a healthy diet, regular exercise, and avoiding excessive caffeine consumption—can help reduce overall migraine frequency and severity.
Healthy eating consistently throughout the day and staying hydrated are two of the most important lifestyle modifications you can make to reduce your symptoms.
Likewise, caffeine can worsen migraine if used too often. People with migraine should consume less than 200mg of caffeine each day.
Both cardiovascular and resistance exercises can help reduce migraine symptoms over time, though they can make an ongoing migraine attack worse.
Supplements
Some supplements can help prevent migraine, including vitamin B2 (riboflavin), CoQ10, and magnesium. Migraine specialists commonly recommend them to reduce how often migraine attacks happen.
Migraine researchers have also studied Butterbur, but you should only use brands that are clearly labeled as PA-free (pyrrolizidine alkaloid-free), because products with PA can be harmful to the liver.
Headache Diary
A headache diary can help you and your care team identify optimal treatment approaches by mapping your specific migraine pattern. The simplest headache diary is called a stoplight diary. It uses a calendar (smartphone-based, a paper flip calendar, or an agenda book) and three colored markers (green, yellow, and red) to illustrate the frequency and severity of symptoms.
- Red Day: A red day is when pain and symptoms are severe enough to prevent daily activities like work, chores, school, and social events. On a red day, you may need to sleep or rest during the attack.
- Yellow Day: A yellow day is when pain and symptoms are mild but still impact you, enabling you to push through some activities. It might be harder to do work, school, chores, or social events.
- Green Day: A green day is when you are 100% pain and headache-free and able to function normally.
- Some people find it helpful to record other important factors, like rescue medications or their menstrual cycle.
Finding the right treatment might take time, so let your healthcare provider know if your migraine symptoms have improved or worsened.
While migraine is a long-term condition, the focus of treatment is on symptom control and improving your quality of life. What’s more, many patients with migraine experience improvement over time or periods of remission, particularly as they get older.
Common Questions
How common is migraine?
Migraine pain and symptoms affect more than 39 million Americans, and nearly 75% people who experience migraine attacks are women. In other words, close to 12% of the U.S. population experiences migraine, and close to 8% of them are women.
Across the globe, 14% of people are affected by migraine, making it one of the most common neurological disorders.
Who gets migraine?
While migraine can affect anyone at any age, you’re more likely to have it if you are female, have a family history of migraine, and have other coexisting conditions.
- Gender differences: Around 18%-20% of women experience migraine, compared to 6%-7% percent of men. This discrepancy is largely thought to be caused by hormones and their fluctuations, particularly changes in estrogen levels.
- Family history: Migraine tends to run in families. In fact, studies have found that up to 80% of people who experience migraine have a first-degree biological relative with the same condition.
- Coexisting conditions: The risk of migraine increases for those with coexisting medical conditions, such as depression, anxiety, bipolar disorder, fibromyalgia, obsessive-compulsive disorder (OCD), sleep disorders, and epilepsy.
What are the most common triggers for migraine?
Migraine triggers aren’t the same for everyone, and it is common to mistake symptoms of the migraine prodrome for triggers. However, commonly reported triggers include:
- Too much or too little sleep
- Sudden weather changes
- Strong odors or fumes
- Stress or other emotions
- Hormonal changes and the menstrual cycle
- Overexertion
- Illness
- Skipping meals
- Tobacco use
- Certain medications or medication overuse
- Specific foods, food additives, and drinks, like processed meats, dark chocolate, aspartame, MSG, and red wine
- Sudden or loud noises
- Bright or flashing lights
It is important to remember that, while triggers can cause symptoms to occur in a person with migraine, they are not the cause of the disease itself.
Can using too much headache medicine cause migraine?
Medication overuse headache occurs when the frequent need for pain-relief drugs causes headaches to become more frequent and severe, sometimes decreasing the response to rescue treatments. It is important to distinguish between medication overuse (MO), which describes taking acute medicine too often, and medication overuse headache (MOH), which describes the brain becoming sensitized to those drugs.
While medication overuse in people with a primary headache disorder like migraine is the main risk factor for developing MOH, not everyone who overuses medicine will develop the condition. However, for some people, frequent use can train the brain to trigger a new headache as the medicine wears off. Medications including triptans, opioids, and combination pills containing caffeine, like Excedrin, can trigger this cycle with as few as 10 days of use per month over at least three months of persistent overuse. Lower-risk medications, such as simple NSAIDs (ibuprofen or naproxen) and acetaminophen (Tylenol), typically require a higher frequency of 15 or more days per month before MOH develops. Researchers have not established a connection between gepants and MOH.
What’s the prognosis for migraine?
Migraine is a chronic condition with no cure, but most people can manage it through medications and lifestyle changes. That said, the overall prognosis varies by individual, depending on a person’s migraine frequency, the degree of their migraine severity, and their response to migraine treatment.
Migraine can change over time and often recedes with age. In fact, many people notice a decrease in migraine attacks after the age of 50—especially women, as hormonal fluctuations related to menstruation, pregnancy, or menopause can influence migraine patterns. However, migraine attacks may worsen or change (for example, you may experience different symptoms) in perimenopause.
Can migraine be prevented?
In addition to preventive medication, the following changes can reduce how severe and frequent your symptoms are:
- Establishing a routine: Consistent meal times, staying hydrated, avoiding too much caffeine consumption (more than 200mg per day), and having a regular sleep pattern can help stabilize your body and reduce the odds of triggering migraine attacks.
- Managing stress: Since stress is a major trigger for migraine, techniques like yoga, meditation, deep breathing exercises, and mindfulness can help to reduce your overall stress levels.
- Exercising regularly: Moderate physical activity, like walking, swimming, or cycling, can help reduce the frequency of migraine attacks by lowering stress and promoting a greater sense of overall well-being. That said, intense exercise can be a migraine trigger, so it’s important to strike the right balance.
Resources
National Institute of Neurological Disorders and Stroke
American Migraine Foundation
News & Stories






Yoga for Migraine

Yoga for Migraine: Head, Neck, Shoulders, and Self Massage

Yoga for Migraine: Meditation

Yoga for Migraine: Body Relaxation

Yoga for Migraine: Full Body Flow


