
Oropharyngeal Cancer
At a Glance
- Oropharyngeal cancer is a type of head and neck cancer that originates in the oropharynx (the throat, including tonsils, base of tongue, soft palate, and pharyngeal walls).
- Common symptoms include a persistent sore throat, difficulty swallowing or speaking, unexplained weight loss, swollen lymph nodes in the neck, ear pain, or changes in voice.
- Diagnosis is typically made through a physical examination, endoscopy with biopsy, and medical imaging studies, often including testing for human papillomavirus (HPV).
- Treatment may include surgery, radiation, and chemotherapy, depending on the cancer’s stage and HPV status.
Overview
Oropharyngeal cancer is a type of head and neck cancer that arises from the oropharynx, which is part of your throat. The middle section of the throat, including the soft palate, the back third of the tongue, the tonsils, and the side and back walls of the throat, make up the oropharynx. It is distinct from oral cancer, which affects the mouth’s structures (the lips, gums, the front two-thirds of the tongue, and the lining of the cheeks and lips).
Risk factors for oropharyngeal cancer include:
- Human papillomavirus (HPV) infection: Infection with certain strains of HPV, especially HPV-16, is by far the leading cause of cancer of the oropharynx. HPV-related oropharyngeal cancers tend to occur in younger individuals and have a better prognosis compared to tobacco-related cancers. Early data suggest that HPV vaccines could help prevent oropharyngeal cancer.
- Number of sexual partners: A higher number of sexual partners could be a risk factor, as number of oral sexual partners has been linked to higher risk of HPV infection and oropharyngeal cancers.
- Tobacco use: The most significant risk factor includes smoking cigarettes, cigars, or pipes, and using smokeless tobacco (chewing tobacco).
- Alcohol consumption: Heavy use of alcohol can increase the risk, and concurrent use of alcohol and tobacco magnifies this risk.
Oropharyngeal cancer symptoms may include a sore throat, swallowing difficulty, a lump in your neck, weight loss, pain or ringing in your ears, or changes in your voice.
Diagnosis is generally made through physical examination, imaging studies (like CT or MRI), and biopsy of the suspicious area. Treatment depends on the stage and location of the tumor. It can include surgery, immune therapy, radiation therapy, targeted therapy, chemotherapy, or a combination thereof. The prognosis and treatment approach can also vary based on whether the cancer is HPV-related or not.
Anatomy of the Throat
The throat is a tube wrapped in muscle that starts behind your nose and mouth and extends down the neck to the larynx (or voice box). You use it to bring air into your lungs and food into your stomach.
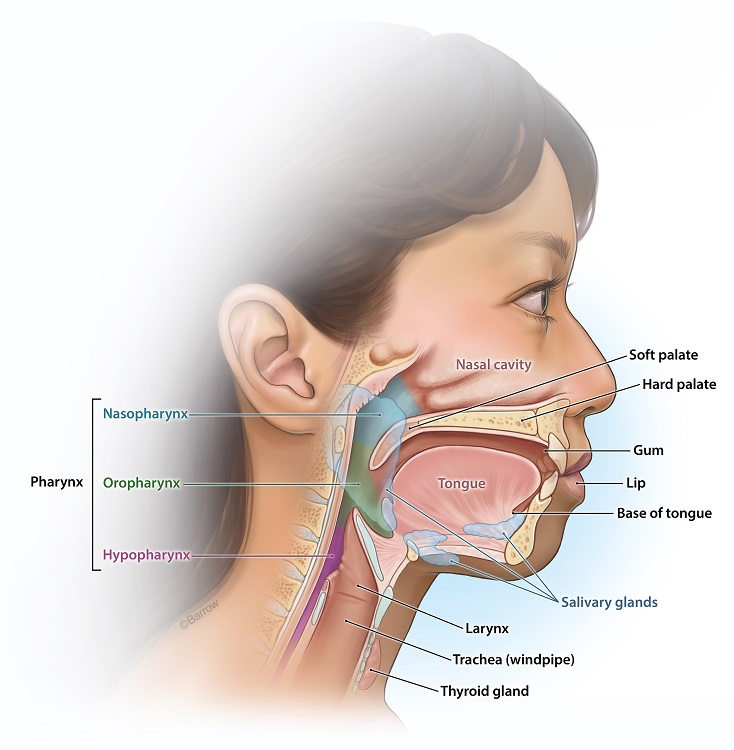
It includes the orpharynx:
- The back of your nose and mouth
- Soft part of the palate/roof of your mouth
- Tonsils
- The back third of the tongue
And also:
- Epiglottis (the flap that prevents solids and liquids from entering your windpipe)
- Voice box (larynx)
- Windpipe (trachea)
- Esophagus

Oropharyngeal Cancer Symptoms
There are many oropharyngeal cancer symptoms, some of which may be mistaken for more common, noncancerous conditions.
Many of these symptoms are caused by conditions other than cancer, such as infections, benign tumors, or other health problems. However, if you or a loved one experiences any of these symptoms, especially if they persist for weeks, it’s crucial to see a healthcare professional for evaluation. Early diagnosis and rapid treatment can improve your prognosis.
Symptoms of oropharyngeal cancer include:
- A persistent sore throat that doesn’t go away for several weeks
- Difficulty swallowing (dysphagia) or feeling like you have something stuck in your throat
- A lump in the back of your mouth, throat, or neck
- Unexplained weight loss
- Pain or ringing in your ears
- Changes in your voice
- Persistent cough
- Coughing or spitting up blood
- Unexplained mouth pain or an ulcer that doesn’t heal
- Swelling or white or red patches
- Difficulty moving the jaw or tongue
- Numbness or weakness in certain areas of the throat or tongue
- Persistent bad breath
- Swollen lymph nodes in the neck
- Breathing difficulties
Diagnosis
Your doctor will use a combination of medical history evaluation, physical examination, and various diagnostic tests and procedures to determine if you have oropharyngeal cancer. Diagnosing oropharyngeal cancer typically involves:
- Medical History and Physical Examination: Your doctor or healthcare provider will conduct a thorough medical history and physical examination. They will ask about your symptoms, risk factors (such as tobacco use, alcohol use, HPV infection, and family history), and any relevant medical conditions.
- Clinical Evaluation: During the physical examination, the healthcare provider will examine your throat, mouth, and neck for any signs of abnormalities, including lumps, masses, or enlarged lymph nodes.
- Biopsy: A definitive diagnosis of oropharyngeal cancer requires a tissue sample (biopsy) from the affected area. This can be done in several ways:
- Fine needle aspiration (FNA): A small sample of tissue or fluid is drawn from a suspicious lump or lymph node using a thin needle.
- Incisional biopsy: A portion of the abnormal tissue is removed for examination.
- Excisional biopsy: In some cases, the entire tumor or suspicious area may be removed for examination.
- Imaging Studies: To determine where the cancer is located, imaging tests (CT, MRI, X-rays) may be ordered.
- Endoscopy: In some cases, an endoscope (a thin, flexible camera) may be used to examine the throat, larynx, and esophagus. This procedure is called a laryngoscopy or pharyngoscopy, and may be done during your initial office visit if oropharyngeal cancer is suspected.
- HPV Testing: If your healthcare provider suspects that the oropharyngeal cancer may be HPV-related, a specific test may be performed to detect the presence of HPV in the tumor tissue.
- Blood Test: HPV related cancers can also often be detected by certain blood tests.
Once the diagnosis is confirmed, additional tests and evaluations will determine the cancer stage, which helps guide treatment decisions. Staging involves assessing the size and spread of the tumor and whether it has invaded nearby tissues or distant parts of your body.
After a definitive diagnosis and staging, a multidisciplinary team of healthcare professionals, including head and neck cancer surgeons, medical oncologists, radiation oncologists, and others, will develop a treatment plan tailored to the specific characteristics of the cancer and your overall health. Treatment options for oropharyngeal cancer may include surgery, radiation therapy, chemotherapy, immunotherapy, or a combination of these approaches.

Oropharyngeal Cancer Treatments
Oropharyngeal cancer treatment options depend on the stage of the disease, the location and size of the tumor, your overall health, and whether it is associated with human papillomavirus (HPV).

Surgery
Surgical removal is often the first and best option for treating oropharyngeal cancer. Different surgical approaches may be used depending on the tumor’s size and location.
Transoral robotic surgery (TORS) and transoral laser microsurgery (TLM) are minimally invasive surgical techniques that use either a robot or a microscope and a laser to remove tumors from the throat through the mouth.
Your head and neck cancer surgeon may remove the lymph nodes in your neck if there is concern that the cancer has spread to them.
Following the removal of larger tumors, free flap microvascular reconstructive surgery may be needed to help restore the structure and function of affected areas.
Radiation Therapy
Radiation therapy uses X-rays, gamma rays, electrons, or protons to bombard cancer cells while attempting to spare healthy tissue nearby. The high energy of these particles makes them lethal to tissue in high doses, so they are directed and concentrated so that only the tumor receives enough radiation to cause damage.
External beam radiation therapy is the most common form of radiation therapy for oropharyngeal cancers.
Chemotherapy
Chemotherapy uses medicines to kill cancer cells or prevent them from growing and dividing. It can be used before surgery to shrink tumors, postoperatively to kill remaining cancer cells, or in combination with radiation therapy.
Immunotherapy
Immunotherapy helps your body’s immune system recognize and attack cancer cells. Some immunotherapy drugs have shown promise in treating head and neck cancers.
Rehabilitation
Due to the location of oropharyngeal cancer, treatments can affect your ability to speak, swallow, and breathe. Rehabilitation may involve speech and swallowing therapy, dietary counseling, and other supportive care measures.
Regular follow-up care after treatment is essential to monitor for recurrence, manage any long-term side effects, and ensure your overall well-being. Your team of specialists will encourage you to discuss the potential benefits and risks of each treatment and help you make informed decisions.
Targeted Therapy
Targeted therapy describes therapeutics that target specific cancer cell proteins or processes without affecting normal cells. Targeted therapies are rarely used for oropharyngeal cancer, with the exception of extremely rare salivary gland cancers of the oropharynx.
Common Questions
Is oropharyngeal cancer curable?
Oropharyngeal cancer can be treated and, in some cases, cured. The chances of a cure depend on several factors, including
- The stage at which the cancer is diagnosed
- The type of cancer
- Your overall health
- The treatment options available to you
In the early stages of oropharyngeal cancer, when the cancer has not spread to the rest of your body, the chances of a cure are generally higher. However, even in more advanced stages, treatment can help manage the cancer, alleviate symptoms, and potentially extend your life.
It’s crucial to detect and diagnose oropharyngeal cancer as early as possible by seeking medical attention for symptoms like persistent hoarseness, difficulty swallowing, ear pain, or a lump in the neck. Catching oropharyngeal cancer early can lead to more effective treatment and better outcomes.
How quickly does oropharyngeal cancer develop?
The development of oropharyngeal cancer can vary significantly from person to person. Oropharyngeal cancer typically develops over years, and the timeline can depend on various factors, including the type of cancer, your risk factors, and genetic predisposition.
In some cases, oropharyngeal cancer may develop from precancerous lesions or conditions like leukoplakia (a permanent white or gray patch of tissue in the throat or mouth) or erythroplakia (a raised, red patch of tissue in the throat or mouth that easily bleeds when touched). These precancerous changes can precede the development of cancer by several years or more. Regular checkups and early intervention can help prevent them from becoming cancerous.
HPV-related oropharyngeal cancers are becoming more common, and they tend to develop more slowly compared to some other types of oropharyngeal cancer.
In short, there is no fixed timeline for how quickly oropharyngeal cancer develops. Anyone experiencing persistent throat or oral symptoms should seek prompt medical attention for evaluation and diagnosis. Early detection and treatment can significantly improve the outlook for individuals with oropharyngeal cancer.
What is the survival rate for oropharyngeal cancer?
Much like the progression of oropharyngeal cancer, the survival rate can vary widely depending on many of the same factors, including the type of cancer, the stage at diagnosis, the specific location of the cancer within the oropharynx, your overall health, and the treatment received. Survival rates are often expressed as percentages and are typically calculated as the proportion of people with a particular type and stage of cancer who are still alive a certain number of years after diagnosis. It’s important to note that these statistics are general estimates and do not necessarily predict your outcome.
Survival rates are typically presented as five-year survival statistics, which is the percentage of people who live at least five years after a cancer diagnosis. The overall five-year survival rate for people with oropharyngeal cancer is around 65%. However, when broken down by stage, the rates varied significantly:
- Localized cancer that has not spread beyond the oropharynx has a five-year survival rate of over 80%.
- Regional cancer that has spread to nearby tissues and/or lymph nodes has a five-year survival rate of 50-60%.
- Distant cancer that has spread to parts of the body far beyond the oropharynx has a five-year survival rate of around 20-30%.
HPV-Positive Survival Rate for Oropharyngeal Cancer
The survival rate for HPV-positive oropharyngeal cancer is generally higher than for oropharyngeal cancers not associated with HPV. Patients with HPV-positive oropharyngeal cancer have a five-year disease-free survival rate of approximately 85% to 90%. This is in contrast to the overall relative survival rates for oropharyngeal cancer, regardless of HPV status (see above).
For the most current statistics and information, it’s best to consult the latest data from cancer registries or health authorities like the American Head and Neck Society, the National Cancer Institute (NCI), the American Cancer Society (ACS), or similar organizations in other countries. Moreover, discussing with your healthcare provider will provide the most personalized and up-to-date information.
What age is oropharyngeal cancer common?
Oropharyngeal cancer can happen at any age, but it is more commonly diagnosed in older adults. The risk of developing oropharyngeal cancer tends to increase as you age. The majority of cases are diagnosed in individuals over the age of 50, and the risk continues to rise as you get older.
HPV related oropharyngeal cancers tend to occur in younger patients, usually male, while smoking and alcohol related malignancies usually arise in older individuals.
What can be mistaken for oropharyngeal cancer?
Several conditions and health issues can cause symptoms that may be mistaken for oropharyngeal cancer. Please consult a healthcare professional if you experience persistent or concerning symptoms. Some conditions that can be mistaken for oropharyngeal cancer include:
- Throat and oral infections, such as tonsillitis, pharyngitis, or a dental abscess, can cause symptoms like sore throat, difficulty swallowing, and swollen lymph nodes in the neck.
- Gastroesophageal reflux disease (GERD) can cause symptoms like chronic heartburn, acid regurgitation, and irritation of the throat and esophagus, which may be mistaken for oropharyngeal cancer.
- Allergic reactions to pollen, dust, or other allergens can lead to throat irritation, coughing, and a scratchy throat.
- Voice disorders like vocal cord nodules, polyps, or laryngitis can result in hoarseness or changes in voice quality, which may be confused with oropharyngeal cancer.
- Benign Tumors and growths in the oropharynx, such as benign tumors or cysts, can cause symptoms like a lump in the throat or difficulty swallowing.
- Thyroid disorders, including thyroid nodules or thyroid cancer, can sometimes cause symptoms in the neck region that might be mistaken for oropharyngeal cancer.
- Certain neurological conditions, such as spasmodic dysphonia or vocal cord dysfunction, can lead to voice changes and difficulty swallowing.
- Medication side effects can cause dry mouth, throat irritation, or voice changes as side effects.
- Physical injury to the oropharynx or voice box can result in symptoms like hoarseness and difficulty swallowing.
- Stress and anxiety can sometimes manifest with symptoms like throat tightness or a feeling of a lump in the throat.
- Lung conditions, such as chronic obstructive pulmonary disease (COPD) or lung cancer, can cause symptoms that may be perceived as throat-related.
- Esophageal conditions, such as achalasia or esophageal strictures, can lead to difficulty swallowing and may be confused with throat issues.
Resources
Patient Stories





References
- Moustafa Mourad, Thomas Jetmore, Ameya A. Jategaonkar, Sami Moubayed, Erin Moshier, Mark L. Urken, Epidemiological Trends of Head and Neck Cancer in the United States: A SEER Population Study, J Oral Maxillofac Surg. 2017 Dec;75(12):2562-2572. doi: 10.1016/j.joms.2017.05.008. Epub 2017 May 22. PMID: 28618252.
- Ameya A. Jategaonkar, Vivian F. Kaul, Eric Lee, Eric M. Genden, Surgery of the Palatomaxillary Structure, SEmin Plast Surg. 2020 May 34(2):71-76. doi: 10.1055/s-0040-1709430. Epub 2020 May 6. PMID: 32390773.
- American Cancer Society. Oral Cavity and Oropharyngeal Cancer Stages. March 23, 2021.
- National Cancer Institute. Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: Oral Cavity and Pharynx Cancer. 2022.