
Spinal Arteriovenous Malformation (AVM)
At a Glance
- A spinal arteriovenous malformation (AVM) is a tangled cluster of blood vessels on or within the spinal cord.
- Spinal AVMs are often congenital, meaning they form during fetal development before birth.
- Symptoms can develop over months or years as the circulation of blood flow to the spinal cord is congested by increased pressure in the veins, or they can appear suddenly if the AVM ruptures and bleeds.
- The most common treatments involve endovascular embolization to block the abnormal arteriovenous connections and/or open neurosurgery to remove the AVM tangle.
Overview
A spinal arteriovenous malformation (AVM) is an abnormal, tangled cluster of blood vessels in and around the spinal cord.
These unusual tangles of blood vessels occur when arteries and veins directly connect without the network of tiny capillaries between them. This arteriovenous connection disrupts the normal flow of blood to the spinal cord, leading to increased pressure in the veins, circulatory congestion, and decreased blood flow, which lowers oxygen delivery to spinal cord tissue. Spinal AVMs can hemorrhage, which can cause permanent neurological damage if left untreated.
While considered rare when compared to brain AVMs, spinal AVMs can develop at any age and can affect all parts of the spinal cord. They are classified based on where they occur and how the atypical artery–vein connections are structured. The four main types of spinal AVMs include:
- Type I—Dural arteriovenous fistula (dAVF): As the most common type of AVM, dural arteriovenous fistulae account for 60% to 80% of all spinal AVMs. They’re located in the tough covering of the spinal cord, called the dura mater, and involve an atypical connection between a radicular artery and a vein. Rather than bleeding, dAVFs tend to cause venous congestion and progressive spinal cord dysfunction.
- Type II—Intramedullary glomus spinal AVM: This type of AVM is located inside spinal cord tissue and is often present from birth, making it congenital. Intramedullary glomus AVMs have a compact tangle of abnormal vessels, called a nidus, fed by one or more arteries. These types of AVMs have a higher risk of bleeding.
- Type III—Juvenile AVM: This complex type of spinal AVM can grow extensively and involve the spinal cord, surrounding meninges, muscle, and vertebrae. Like Type II AVMs, juvenile AVMs are almost exclusively congenital, meaning they mostly appear in children or young adults, and can cause severe, early-onset symptoms. Juvenile AVMs are often challenging to treat due to their size and their involvement of multiple structures.
- Type IV—Intradural perimedullary arteriovenous fistula (pAVF): This type of spinal AVM is located on the surface of the spinal cord, called the pia mater. A pAVF has a direct artery-to-vein shunt on the surface of the spinal cord supplied by a single artery, rather than a compact tangle of blood vessels. pAVFs are more likely to occur in younger individuals and can present with rupture or subarachnoid hemorrhage.

What causes Spinal AVMs?
The exact cause of spinal AVMs is not fully understood, but researchers believe most are congenital, meaning they form during fetal development, before birth. Usually, an intricate network of capillaries connects arteries and veins in the spinal cord. This capillary network slows blood flow and allows oxygen and nutrients to permeate nearby tissue while removing carbon dioxide and waste products.
In these cases, an error in the formation of blood vessels results in arteries connecting directly to veins without capillaries, creating high-pressure, fast-flowing channels.
Though much less common, some spinal AVMs may develop later in life from spinal cord trauma, inflammation or infection, tumors, or conditions affecting blood vessel health.
There is no substantial evidence that they run in families, so spinal AVMs are generally not considered hereditary.
Did you know?
Since AVMs are the result of abnormal connections between veins and arteries that become entangled, they can happen anywhere in the body—not just the spinal cord.
Spinal AVM Symptoms
The symptoms of spinal arteriovenous malformations vary, depending on their exact location, size, and the extent of blood flow through the malformation.
Symptoms can occur gradually over months or years, as the spinal cord is slowly deprived of oxygen, or appear suddenly if a vessel ruptures and bleeds. Most often, individuals don’t even know they have a spinal AVM. Instead, they’re found during a treatment or diagnosis for another condition.
Symptoms of a spinal AVM can include:
- Weakness in the legs or arms: This can be a gradual or a sudden loss of strength, often starting in the legs and sometimes progressing upward. You may also experience heaviness in the legs or arms and poor coordination or unsteadiness.
- Numbness or tingling: Unusual sensations, like pins-and-needles, tingling, burning, or a complete loss of feeling in parts of the body below the location of the spinal AVM, can occur.
- Back pain: A persistent or sudden sharp pain, usually in the mid- or lower back near the spinal AVM, is common. This pain may also radiate along nerve pathways.
- Muscle stiffness or spasms: Increased muscle tone, known as spasticity, or an involuntary tightening of muscles, can make movement challenging.
- Loss of bladder or bowel control: Poor nerve signaling to the bladder can lead to trouble starting urination, an inability to fully empty the bladder, or a complete loss of control. Poor nerve signaling to the bowels can cause constipation or bowel incontinence.
- Sexual dysfunction: Due to nerve involvement, reduced sexual sensations can occur. Women may have trouble reaching orgasm, while men may experience erectile dysfunction.
- Sensory changes to temperature or pain: An inability to sense hot, cold, or painful stimuli in the affected areas of your body can increase your risk of injury.
- Progressive paralysis: When an AVM continues to impair spinal cord function, muscle weakness can worsen and lead to progressive paralysis.
- Sudden, severe neurological changes: A rapid onset of numbness, weakness, or paralysis can happen if your AVM bleeds.
Any new or unexplained symptoms mirroring those outlined above need to be evaluated by a healthcare professional as soon as possible. Without diagnosis and treatment, the risk of lasting spinal cord injury is significant.
Spinal AVM Diagnosis
Diagnosing a spinal arteriovenous malformation (AVM) often requires a combination of evaluation and specialized imaging, because its symptoms can mimic other spinal cord disorders.
Your doctor might use the following exams, tests, and imaging studies to diagnose a spinal AVM:
- Physical and neurological examination: Your healthcare provider will ask about your symptoms, overall health, and history of trauma or infection. Next, they’ll complete an exam to assess your neurological function, including your reflexes, coordination, strength, sensation, and potential signs of spinal cord dysfunction. While this step can suggest that a spinal cord problem exists, it cannot confirm a spinal AVM.
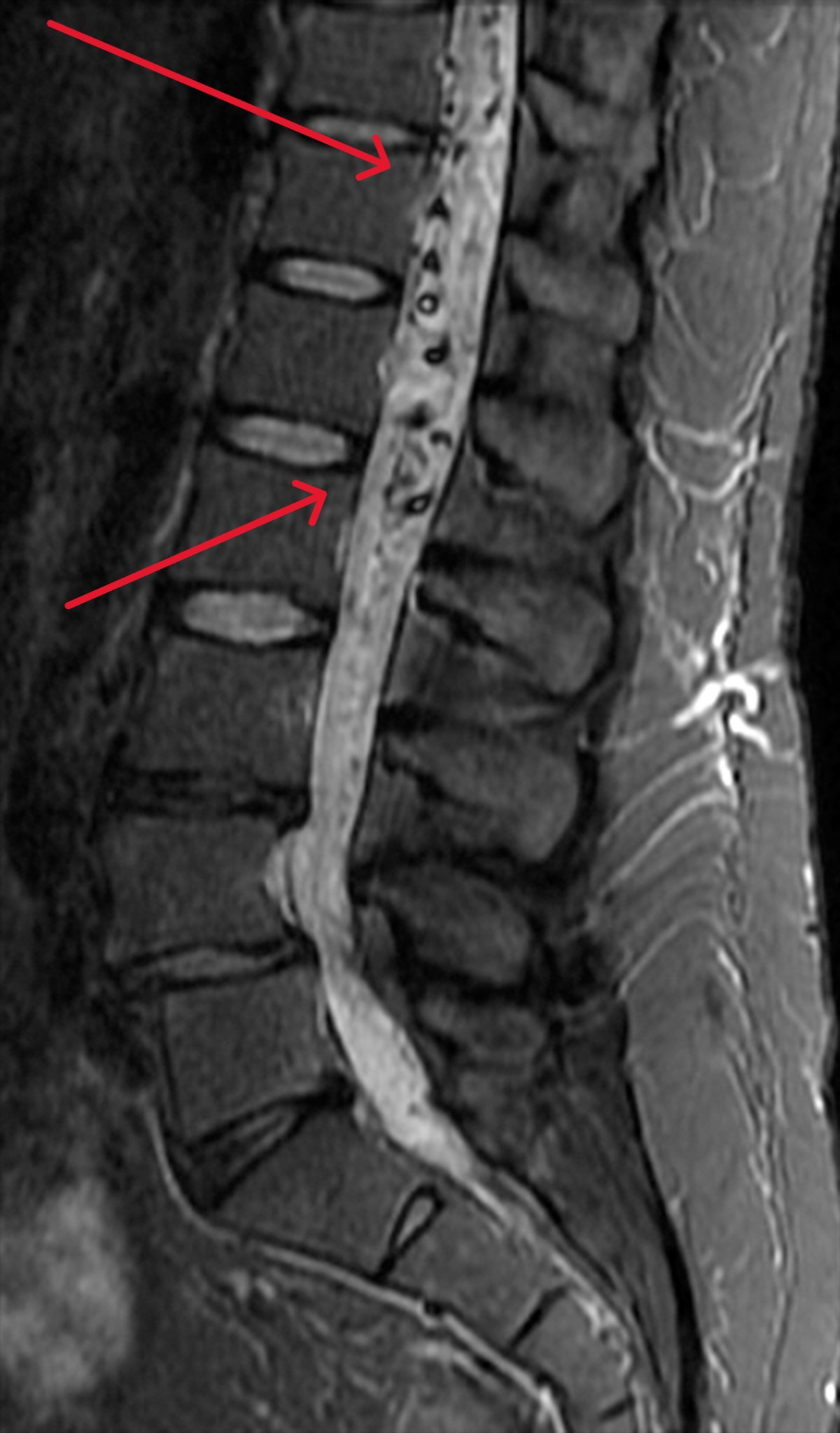
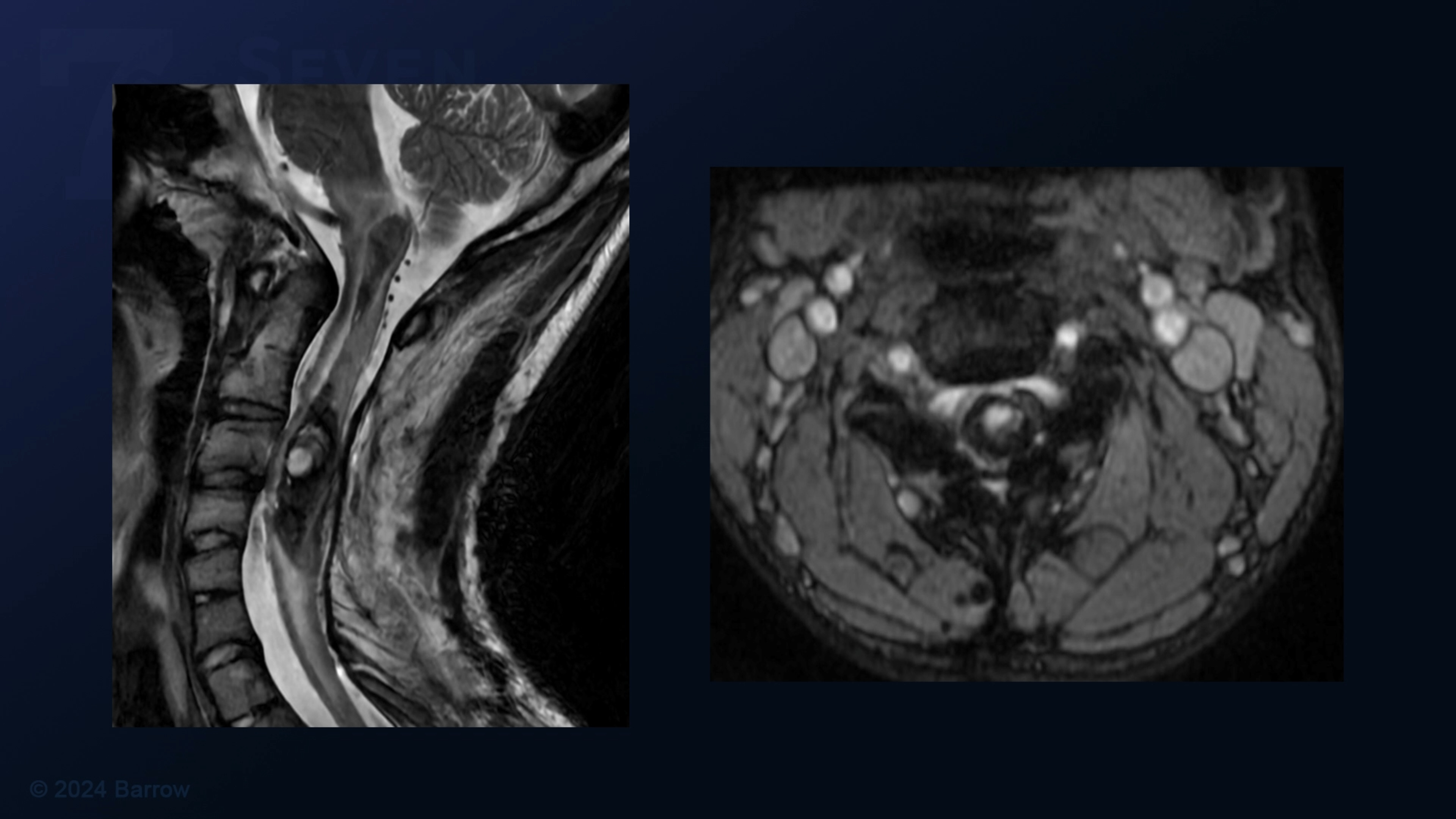
- Magnetic Resonance Imaging (MRI): Imaging studies are crucial in visualizing the spine and spinal cord and identifying any abnormalities. An MRI can reveal areas where blood is moving rapidly, swelling of the spinal cord, or evidence of bleeding.
- Computed Tomography (CT) scan: If an MRI isn’t advised, a CT scan may be done to look for calcifications or bleeding. However, CT scans are less sensitive than an MRI.
- Magnetic Resonance Angiography (MRA): This contrast-enhanced MRI scan can provide detailed images of blood vessels to see how blood flows through the body, improving the detection of abnormal vessels. This, in turn, reveals an AVM’s location and size. A contrast dye is sometimes injected to help blood vessels stand out further, though an MRA can also be done without contrast.
- Spinal Angiography: Considered the gold standard in diagnosing spinal AVMs, spinal angiography provides an in-depth look at the blood vessels of the spinal cord and its surrounding structures. During the procedure, a thin catheter is inserted through the groin and threaded into the arteries that supply the spinal cord. Contrast dye is then injected, and X-ray images are taken in rapid sequence to track blood flow and highlight any abnormalities. Spinal angiography is essential to confirming the diagnosis of a spinal AVM.
- Lumbar puncture: If bleeding is suspected, a lumbar puncture may be done, although this diagnostic tool is increasingly uncommon with advances in imaging. A lumbar puncture involves a needle inserted into your lower back to collect cerebrospinal fluid (CSF) to check for blood, which may indicate a spinal AVM.

Spinal AVM Treatments
The main goal of spinal arteriovenous malformation (AVM) treatment is to eliminate blood flow to the malformation, stop further spinal cord injury, and allow neuronal function in the spinal cord to recover.

Minimally Invasive Treatments
Less invasive options can help stabilize spinal AVM symptoms, but they don’t always cure them. Whether your neurosurgeon recommends nonsurgical treatment for you will depend on the type of spinal AVM, its location, size, and symptoms.
Minimally invasive approaches include:
- Endovascular embolization: In this procedure, a catheter is guided through the network of arteries until it reaches the AVM. Various branches to the AVM are then plugged with an embolic agent—a substance or material that blocks blood flow—to close the abnormal vessels and reduce blood flow. This, in turn, quiets the AVM and makes it safer to remove during surgery. Endovascular embolization can be used as a stand-alone treatment or alongside microsurgical resection.
- CyberKnife Radiosurgery: Although not commonly used for spinal AVMs, radiosurgery relies on focused radiation beams targeted at the AVM while minimizing radiation to the rest of the spinal cord. Over time—typically 3 years—the AVM’s arteries respond to the radiation by scarring and closing down. Because the full effects of radiosurgery can take months to years to happen, it’s not suitable for urgent cases.
- Medications: If an AVM is small and asymptomatic, or the risks of an intervention outweigh the benefits, your doctor might recommend careful management through medications. Multiple medications can help relieve the symptoms of an AVM, including:
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- Neuropathic pain medications like gabapentin, pregabalin, or duloxetine
- Medications to reduce muscle spasticity, like baclofen or diazepam
- Blood pressure management medications
- Drugs to improve bladder function or bowel regulation

Microsurgical Resection
Many spinal AVM cases require surgery to remove or disconnect the malformation and prevent further spinal cord injury or bleeding.
As the leading surgical treatment for an arteriovenous malformation, microsurgical resection is generally most effective for small to moderate-sized AVMs. In this procedure, a neurosurgeon performs an open surgery using an operating microscope to remove the AVM or disconnect its abnormal blood vessels carefully. This approach works best for accessible lesions where complete removal is safe without damaging healthy cord tissue.
In some instances, instead of removing the entire AVM, your neurosurgeon will disconnect the abnormal arteries feeding it, which stops the high-pressure blood flow to the nidus. Neurosurgeons use this technique for larger, more extensive spinal AVMs that are too risky to remove entirely.

Neuro-Rehabilitation for Quality of Life
At Barrow Neurological Institute, our patients have access to various neuro-rehabilitation specialists to maximize independence. Neuro-rehabilitation can include physical therapy to help you regain strength and balance, speech therapy to support speaking, expressing thoughts, or swallowing, and occupational therapy to aid you in managing daily activities like bathing, dressing, and using the bathroom.
Videos: Surgical Treatment of Spinal AVMs
Warning: Contains surgical footage. Viewer Discretion is advised.


Common Questions
How common are spinal AVMs?
Spinal AVMs are considered very rare. However, the exact numbers are hard to know because many cases go undiagnosed until symptoms are significant or bleeding occurs.
Because spinal AVM symptoms can mimic other spinal disorders like a herniated disc or multiple sclerosis (MS), diagnosis is often delayed. This, in turn, makes estimating the prevalence of the condition tricky.
In the United States, studies suggest an incidence of between 300 and 500 new cases annually, or less than one case per 100,000 people per year. Globally, spinal AVMs could occur in approximately 3 to 10 people per one million people.
Who gets spinal AVMs?
Spinal AVMs can occur in almost anyone, but researchers have identified specific patterns in available data:
- Intramedullary spinal AVMs, or AVMs inside the spinal cord tissue, are often congenital and appear earlier in life. Most patients are diagnosed between their teens and forties, with a peak in the twenties or thirties, and they affect men and women about equally.
- Spinal dural arteriovenous fistulas (dAVFs), the most common type of spinal AVM, are generally acquired and diagnosed later in life, between the ages of 40 and 60. They’re much more common in men, and doctors think they’re influenced by hormonal and vascular factors, as well as small injuries, thrombosis, or degenerative changes in the spine over time.
Across all types of spinal AVMs, there is a slight male predominance, but this is mainly due to the higher incidence of spinal dural arteriovenous fistulas (dAVFs) in men. There’s no strong evidence that race or ethnicity affects spinal AVM risk, as most cases are sporadic and without family history. That said, rare genetic vascular disorders, like hereditary hemorrhagic telangiectasia (HHT), can predispose an individual to AVMs.
What is the prognosis for someone with a spinal AVM?
The prognosis for someone with a spinal AVM depends on several factors: the type of AVM, its size and location, whether it has bled, and whether it is treated soon after detection.
With timely treatment—whether that’s surgical removal, endovascular embolization, or a combination of the two—the outlook improves. Many patients recover fully and stabilize or experience a partial recovery of strength, sensation, and bladder or bowel control. However, a complete recovery is less likely if spinal AVM symptoms have been present for a long time before treatment, or if there’s been a major hemorrhage.
Without treatment, the natural course of a spinal AVM is to worsen progressively. The abnormal vessels can rob the spinal cord of oxygen or bleed, leading to permanent nerve damage. This can cause weakness, numbness, difficulty walking, and loss of bladder or bowel control. Spinal AVMs themselves are rarely fatal, but they can lead to permanent disability when untreated. Between 50% and 70% of patients will develop a significant disability within three to five years of symptom onset if not treated, especially in the case of dural AVFs.
Can spinal AVMs be prevented?
Generally, it is not possible to prevent spinal AVMs, as most are congenital. This means they have formed during fetal development, before birth. There are no known lifestyle changes, medications, or interventions that can stop them from developing, and they don’t typically run in families.
The best strategy for spinal AVMs is early detection and intervention, which can look like:
- Seeking prompt medical evaluation for unexplained weakness, numbness, gait changes, or bladder and bowel problems
- Undergoing imaging protocols when your symptoms suggest atypically formed blood vessels in the spinal cord
- Following up on any abnormal imaging findings rather than delaying care.
Resources
The Aneurysm and AVM Foundation


