
Stroke
Overview
A stroke occurs when there’s a sudden loss of blood flow to the brain due to a blood vessel blockage or rupture. This loss of blood flow deprives brain cells of oxygen, and they begin to die within minutes—meaning the functions these brain cells control are impaired or lost entirely. In other words, neurologists and neurosurgeons have a critical window of minutes to diagnose and treat a stroke.
Broadly speaking, there are two categories of stroke: ischemic stroke and hemorrhagic stroke. An ischemic stroke happens when fatty deposits build up inside a blood vessel that supplies blood to the brain or when a blood clot travels to the brain, blocking blood flow. A hemorrhagic stroke occurs when a blood vessel leaks or ruptures, leading to bleeding in or around the brain and compressing or damaging brain cells.
Strokes can be further categorized as follows:
- Intracerebral hemorrhage: Another type of hemorrhagic stroke, an intracerebral hemorrhage happens when a blood vessel bleeds or ruptures, leaking blood into the surrounding brain tissue within the brain.
- Subarachnoid hemorrhage: This is defined by bleeding between the brain and the thin tissues that cover it, known as the subarachnoid space. A ruptured brain aneurysm is the usual cause.
- Intraventricular hemorrhage: This describes a hemorrhagic stroke that causes bleeding into the open spaces in the brain that contain cerebrospinal fluid (CSF). It is much less common than intracerebral and subarachnoid hemorrhages.
- Embolic stroke: This type of ischemic stroke occurs when a blood clot or other debris forms elsewhere in the body—often the heart—and travels to the brain, blocking blood flow.
- Thrombotic stroke: This type of ischemic stroke happens when a blood clot forms in one of the arteries supplying blood to the brain or inside an artery within the brain.
- Transient ischemic attack (TIA): Also known as a “mini stroke,” a TIA is a disturbance in brain function caused by a temporary blockage of blood to the brain that resolves. While there is usually no permanent injury to the brain, it’s a warning sign that a major stroke may soon occur.
- Cryptogenic stroke: This type of stroke has no clear or definite cause and is only identified when other causes are ruled out. Most cryptogenic strokes result from a blockage in blood flow to the brain, meaning they meet the definition of an ischemic stroke.
- Brain stem stroke: A brain stem stroke occurs when the blood supply to the brain stem is interrupted by a clot or bleeding. The brain stem controls vital functions like breathing, heartbeat, consciousness, and basic motor pathways. When a brain stem stroke happens, it can affect both sides of the body and may leave a person unable to speak or move below the neck.
When to call 9-1-1: Any kind of stroke can be life-threatening and warrants immediate medical attention.
If you or someone around you experience the sudden onset of a ‘thunderclap headache’ (often described as the worst headache of your life), paralysis of the face or other body parts, coordination or balance issues, nausea and vomiting, incontinence, or light sensitivity (photophobia), call 9-1-1 and wait for help to arrive.
What causes a stroke?
For ischemic strokes, the most common risk factor is high blood pressure, known as hypertension. Other leading causes include:
- Atherosclerosis, or the buildup of fatty deposits or plagues in the arteries
- Blood clots
- Heart conditions like atrial fibrillation or irregular heartbeat
- Heart valve disease
- Blood disorders like sickle cell disease, inflammation of blood vessels, or even severe dehydration can also increase the risk of stroke.
Hemorrhagic strokes are commonly caused by hypertension, aneurysms, arteriovenous malformations (AVMs), trauma or head injury, or overuse of blood-thinning medications like warfarin or aspirin. Amyloid angiopathy, a condition where protein deposits in blood vessel walls increase the risk of bleeding, is also a common hemorrhagic stroke cause in older adults.


There’s also a high risk of hemorrhagic stroke following an ischemic stroke. Called a hemorrhagic conversion, the risk of hemorrhagic stroke increases dramatically in the days (up to two weeks) after a large ischemic stroke.
In addition to these causes, modifiable and non-modifiable risk factors can increase your likelihood of a stroke. Modifiable risk factors, or risk factors for stroke that you can influence or change, include:
- Uncontrolled high blood pressure
- Diabetes or high cholesterol
- Smoking and excessive alcohol use
- Poor diet, particularly one high in salt, sugar, and saturated fats
- Obesity and a sedentary lifestyle
Factors that you cannot influence or change, called non-modifiable risk factors, include:
- Your age and gender: The risk of stroke increases with age, and women are at a slightly higher lifetime risk of stroke than men.
- Your genetic predispositions: A family history of stroke or vascular disease affects stroke likelihood.
- Your race: People of African American or Hispanic descent have a higher stroke risk, in part due to higher rates of hypertension and diabetes.
Regular check-ups with your healthcare team can help you recognize and manage these risk factors and significantly reduce stroke risk.


Stroke Symptoms
The signs of a stroke depend on which side of your brain is affected, the structure or structures of the brain affected, and the severity of the stroke. This means that each person may experience different warning signs.
However, stroke symptoms typically appear suddenly and call for immediate medical attention. If you think you’re having a stroke or even a “mini stroke” or transient ischemic attack (TIA), call 9-1-1 immediately.
Someone having a stroke may experience the following symptoms:
- Sudden, severe headache, sometimes referred to as a “thunderclap headache” or “the worst headache of my life”
- Paralysis or weakness on one side of the body
- Sudden numbness, weakness, or tingling
- Confusion and difficulty speaking or understanding speech
- Vision problems
- Dizziness or vertigo
- Chest pain or shortness of breath
- Nausea or vomiting
- Difficulty walking or loss of balance
- Sudden vision problems in one or both eyes

Recognizing a stroke quickly and calling 9-1-1 leads to faster diagnosis, treatment, and better recovery. People should “BE FAST” when it comes to stroke.
Here’s how to BE FAST:
- B – BALANCE: Ask the person to walk. Do they have trouble keeping their balance or walking normally?
- E – EYES: Ask the person about their eyesight. Have they lost vision or experienced vision changes in one or both eyes?
- F – FACE: Ask the person to smile. Does one side of the face droop?
- A – ARMS: Ask the person to raise both arms. Does one arm drift downward?
- S – SPEECH: Ask the person to repeat a simple phrase. Is their speech slurred or strange?
- T – TIME: If you observe any of these signs, call 9-1-1 immediately.
Stroke Diagnosis
It’s critical to determine whether a stroke is hemorrhagic or ischemic as soon as possible because the treatment will be different for each. Brain imaging should be done immediately upon hospital arrival or curbside in a mobile stroke unit to confirm the diagnosis. Ideally, diagnosis happens within 60 minutes or less from when the symptoms are first noticed.
If you have symptoms of a stroke or a transient ischemic attack (TIA), your care team will perform several of the following to reach a diagnosis quickly:
- Physical and neurological exam: Your healthcare provider will ask about your symptoms, overall health, and family history of stroke or related conditions. Next, they’ll complete a neurological examination to assess your neurological function, including reflexes, coordination, strength, and sensation.
- Cerebral angiography: The gold standard for detecting vascular lesions, cerebral angiography uses a special dye and X-rays to take detailed images of the blood vessels in the brain. A thin tube is inserted into an artery, usually in the leg, and guided up to the brain to deliver the dye. This allows doctors to see issues like a burst blood vessel, aneurysm, or abnormal vessel formation. It’s invaluable in diagnosing the cause of a hemorrhagic stroke and planning the best treatment.
- Electrocardiogram (ECG): An electrocardiogram is a simple and timely test that records electrical signals in the heart and can detect irregular heart rhythms.
- Echocardiogram: Also known as an “echo,” an echocardiogram is a non-invasive imaging test that uses ultrasound waves to create detailed pictures of the heart and its structure, function, and movement.
- Magnetic resonance angiography (MRA): Magnetic resonance angiography relies on MRI technology to produce detailed images of the blood vessels
- Blood tests: These include a complete blood count (CBC) to check for infection, clotting issues, or anemia; coagulation tests to assess blood clotting ability; glucose levels to rule out hypoglycemia; lipid panels to check cholesterol; and markers for infectious or clotting disorders.
- Lumbar puncture: Also known as a spinal tap, a lumbar puncture is not routinely used to diagnose a stroke but may be done in specific cases where additional information is needed to clarify the diagnosis—particularly when there’s suspicion of a subarachnoid hemorrhage or another condition mimicking stroke. A lumbar puncture involves a needle being inserted into the lower part of the spinal canal to collect cerebrospinal fluid (CSF) for analysis.
Ideally, an initial assessment is completed within 10 minutes. Within 25 minutes, an MRI or CT scan is done. And in 60 minutes or less, a diagnosis is made and treatment is initiated.
Our team at Barrow Neurological Institute’s Petznick Stroke Center can perform a full range of diagnostic tests to determine the exact cause of a stroke 24 hours a day, seven days a week.

Stroke Treatment
Treatment for a stroke depends on the type of stroke experienced and its severity. However, doctors can minimize the impact of a stroke by delivering the appropriate care within the first four hours and 30 minutes of the onset of symptoms. The longer a stroke goes untreated, the more brain cells die, and the more difficult recovery becomes.
The primary goals of stroke treatment are to restore blood flow to the brain, prevent further damage, and manage underlying risk factors to reduce recurrence.
Treatments for Ischemic Stroke
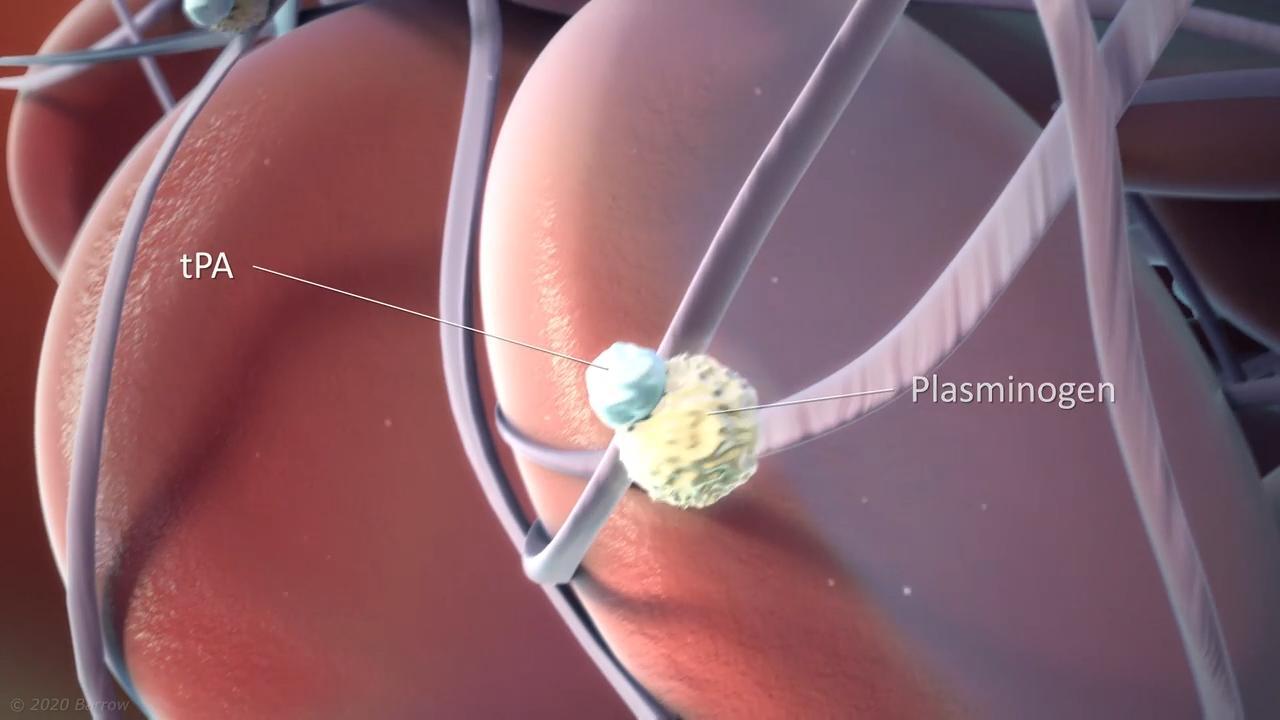
- Thrombolytic therapy: For the first 4.5 hours after a stroke, IV administration of a “clot-busting” medication called tenecteplase (TNK) can dissolve the blood clot and restore crucial blood flow to the brain. However, to be effective, doctors must give this treatment within 4.5 hours of the last time a person was known to be well. This is because TNK doesn’t improve outcomes after the first 4.5 hours of symptoms appearing.
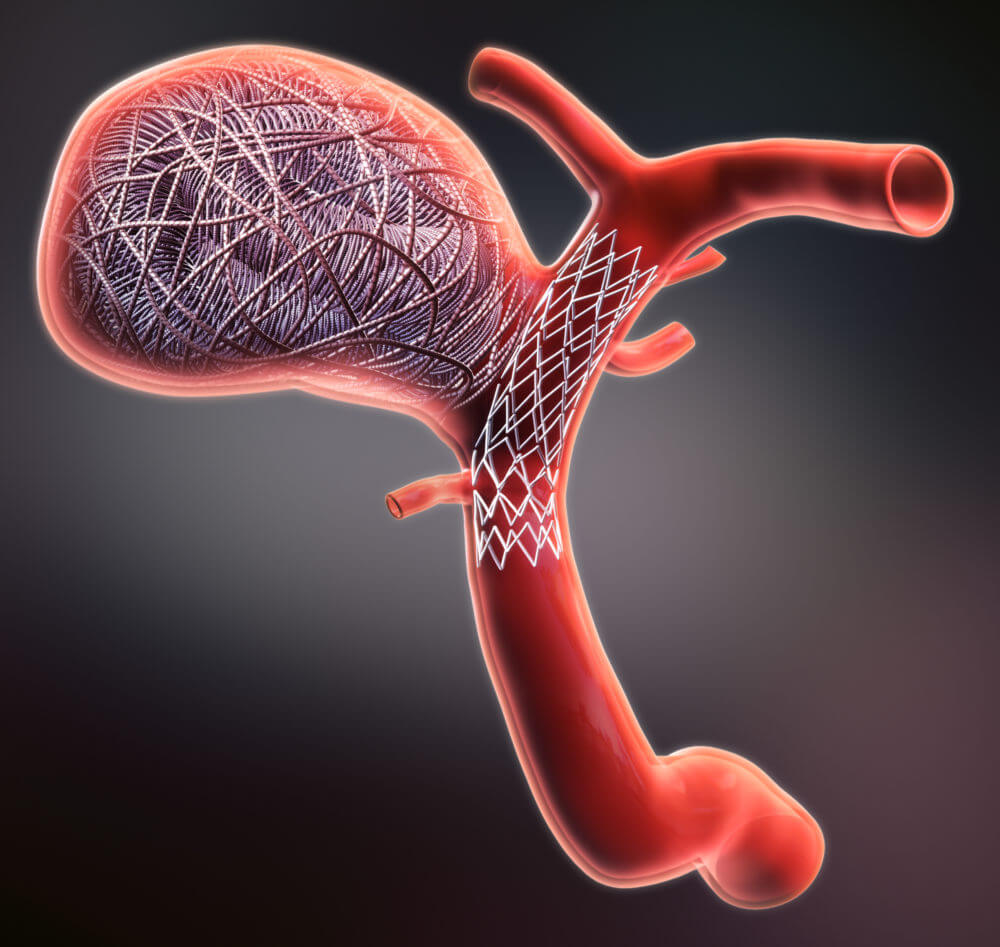
- Thrombectomy: Thrombectomy therapy: Doctors may use this minimally invasive surgical procedure when a large artery blockage causes a stroke. In this procedure, a surgeon mechanically removes the blood clot by breaking it up and removing the pieces through a catheter or retrieving it with a stent device. However, this treatment must be done within 24 hours of the onset of symptoms.
- Carotid endarterectomy: This surgical procedure removes plaque buildup from the carotid arteries, or large blood vessels in the neck that supply blood to the brain, face, and head, and reduces the risk of future strokes.
- Angioplasty: This is a minimally invasive medical procedure used to open narrowed or blocked blood vessels and restore proper blood flow. In this procedure, a balloon is used to widen the narrowed arteries, and if needed, a stent—or small, wire mesh tube—is placed to keep them open.
- Antiplatelet therapy: Medications like aspirin, clopidogrel, or dipyridamole can be administered to prevent platelets from clumping together and forming new clots, reducing the risk of additional strokes.
- Anticoagulant therapy: Doctors may prescribe blood thinners like warfarin or direct oral anticoagulants (DOACs) to prevent new or existing clots from growing in people with conditions like atrial fibrillation.
- Blood pressure management: Since high blood pressure is the most common risk factor for stroke, medications to lower or stabilize blood pressure are often an essential part of treatment.
- Cholesterol-lowering drugs: Drugs like statins play a crucial role in managing stroke risk by lowering cholesterol levels and improving outcomes after a stroke.
- Anti-seizure medications: If a stroke causes seizures or there’s a high risk of them occurring, your doctor may prescribe anti-seizure medications.
- Blood sugar control: Maintaining optimal blood glucose levels with insulin or oral medications reduces the risk of stroke complications and further damage for those with diabetes.
Treatments for Hemorrhagic Stroke
It’s critically important to treat hemorrhagic stroke quickly to save as much brain tissue as possible.
The first phase of treatment is dedicated to stabilizing a person’s vital signs and stopping bleeding in the brain. If you’re taking blood thinners (antithrombotic medications such as apixaban or aspirin) and have a hemorrhagic stroke, doctors may give you reversal agents to quickly stop the blood-thinning effect. This helps reduce further bleeding in the brain and lowers the risk of complications. In some cases, surgery may be needed to remove the clotted blood that’s putting pressure on the brain, to place a temporary drainage catheter to reduce pressure within the brain, or to repair the ruptured artery.
- Endovascular surgery: This treatment is a minimally invasive surgical procedure that uses a tube called a catheter, and devices passed through arteries in the arm or leg to repair the weak spot or break in a blood vessel, like an aneurysm or ruptured arteriovenous malformation (AVM). The catheter is then used to repair the damage and prevent further bleeding.
- Endovascular embolization: Also known as coiling, a catheter is used to place coils inside an aneurysm, promoting clotting and sealing off the weakened area of the blood vessel.
- Aneurysm clipping: In this procedure, a small clip is placed at the base of an aneurysm to isolate it from normal blood circulation, preventing it from rupturing or bleeding again if it bursts.
- Craniotomy for hematoma evacuation: During this procedure, a portion of the skull is removed—known as a craniotomy—to access and clear out pooled blood, called a hematoma, that compresses brain tissue. This, in turn, relieves the pressure caused by swelling or bleeding.
- Arteriovenous malformation (AVM) surgery: This is the removal or repair of an abnormal tangle of blood vessels in the brain that leads to high-pressure arterial blood flowing directly into veins without the usual capillary network in between. In this process, surgery, embolization, or radiation therapy may be used to repair the abnormal blood vessels that caused the hemorrhage to prevent further bleeding and alleviate complications.
- Blood pressure management: Since high blood pressure is the most common risk factor for stroke, medications to lower or stabilize blood pressure are often an essential part of treatment.
- Cholesterol-lowering drugs: Drugs like statins play a crucial role in managing stroke risk by lowering cholesterol levels and improving outcomes after a stroke.
- Blood sugar control: Maintaining optimal blood glucose levels with insulin or oral medications reduces the risk of stroke complications and further damage for those with diabetes.
- Anti-seizure medications: If a stroke causes seizures or there’s a high risk of them occurring, your doctor will prescribe anti-seizure medications.
Emerging Stroke Treatments
Emerging treatments for stroke are working to extend the window of treatment, minimize brain damage, and improve recovery. While many are still in the experimental stage, they’re hopeful indicators for improving outcomes and quality of life for those who have experienced a stroke. Emerging treatments for stroke include:
- Stem cell therapy: Research is ongoing, and scientists are studying stem cells for their potential to replace damaged brain cells, promote regeneration of neural networks, and release growth factors that enhance recovery.
- Neuroprotective agents: These medications protect brain cells from damage during the acute phase of a stroke and reduce damage. Examples include NMDA receptor antagonists, free radical scavengers, and anti-inflammatory agents.
- Nanotechnology: Researchers are investigating using nanoparticles to deliver drugs directly to the brain, such as thrombolytic therapies or neuroprotectants, enhancing their effectiveness and minimizing the side effects of stroke.
- Hemostatic agents: These innovative new drugs that work to stop bleeding rapidly are being tested to minimize brain damage in hemorrhagic strokes.
Early recognition and swift medical intervention are critical to effectively leveraging these emerging treatments.
One Central Location with Multiple Treatment Options
At the Petznick Stroke Center at Barrow Neurological Institute, we’re dedicated to best-in-class stroke care and exhaustive research to find new ways to treat and prevent stroke. Our Center cares for more stroke victims than any other center in the southwestern U.S. We’re also a leading stroke research center, conducting more clinical and prevention trials than any other institution in the region.
From curbside care in our mobile stroke unit to reintegration into the community after a stroke, our Petznick Stroke Center offers a complete spectrum of care for you or your loved one.
Neuro-Rehabilitation for Quality of Life
Neuro-rehabilitation is key to stroke recovery. While it doesn’t reverse brain damage, neuro-rehabilitation can help stroke patients achieve the best long-term outcome possible.
Rehabilitation treatments will vary, depending on the part of the brain affected and the severity of stroke. Treatments can be provided in an acute care hospital, a rehabilitation hospital, or an outpatient setting. At Barrow Neurological Institute, our CARF-accredited Neuro-Rehabilitation Center offers inpatient, outpatient, and transitional rehabilitation programs. We also lead the industry in using neuro-robotics. These cutting-edge technologies allow patients to reach unprecedented heights in function and independence.
Lastly, it’s important to remember that after a stroke, depression and anxiety have a greater likelihood of developing: about one in three people in the first year develop depression, while one in four develop anxiety. While it’s easy to focus solely on the physical recovery, your emotional health is equally important. Please get in touch with your healthcare provider if you suspect you or someone you love may be struggling with either condition.
Common Questions
How common are strokes?
Stroke is the leading cause of severe long-term disability in the United States. It’s also the fifth leading cause of death overall.
More than 795,000 Americans suffer a stroke every year, and of that number, close to 140,000 people do not survive. In other words, nearly 18% of Americans who experience a stroke do not live.
Who is likely to experience a stroke?
The prognosis for someone who has had a stroke depends on multiple factors, including the type of stroke, its severity, the area of the brain affected, how quickly treatment was received, and a person’s overall health. Some individuals recover fully, while others may experience long-term or permanent disabilities.
In ischemic strokes, the prognosis tends to be better than in hemorrhagic strokes. Early treatment with clot-busting drugs or thrombectomy therapy significantly improves outcomes. Generally speaking, hemorrhagic strokes are more likely to be associated with long-term disabilities and higher mortality rates. What’s more, between 10% to 20% of stroke patients die within the first month of experiencing a stroke.
Some individuals regain all pre-stroke abilities, especially following mild strokes or those with timely treatment. Many stroke survivors experience a partial recovery, meaning they can have lasting impairments, like weakness or paralysis on one side, difficulty with balance, coordination, or swallowing, or speech and language problems. In some cases, strokes result in severe disability, such as memory loss or reduced executive function and dependence on caregivers for daily activities.
As a whole, faster treatment for all strokes leads to better outcomes. So, too, does the effective management of modifiable risk factors, like high blood pressure or obesity.
What is the prognosis for someone who experiences a stroke?
The prognosis for someone who has had a stroke depends on multiple factors, including the type of stroke, its severity, the area of the brain affected, how quickly treatment was received, and a person’s overall health. Some individuals recover fully, while others may experience long-term or permanent disabilities.
In ischemic strokes, the prognosis tends to be better than in hemorrhagic strokes. Early treatment with clot-busting drugs or thrombectomy therapy significantly improves outcomes. Generally speaking, hemorrhagic strokes are more likely to be associated with long-term disabilities and higher mortality rates. What’s more, between 10% to 20% of stroke patients die within the first month of experiencing a stroke.
Some individuals regain all pre-stroke abilities, especially following mild strokes or those with timely treatment. Many stroke survivors experience a partial recovery, meaning they can have lasting impairments, like weakness or paralysis on one side, difficulty with balance, coordination, or swallowing, or speech and language problems. In some cases, strokes result in severe disability, such as memory loss or reduced executive function and dependence on caregivers for daily activities.
As a whole, faster treatment for all strokes leads to better outcomes. So, too, does the effective management of modifiable risk factors, like high blood pressure or obesity.
Can strokes be prevented?
The good news is that most strokes are preventable. Approximately 80% of all strokes can be prevented by lifestyle and behavior modification and control of healthcare conditions like diabetes, obesity, and high cholesterol.
If you have any of the following risk factors, please speak with your healthcare provider to come up with a plan to reduce your risk:
- High blood pressure, specifically systolic blood pressure greater than 140 mm/Hg and diastolic blood pressure greater than 85 mm/HG.
- Smoking
- Excessive alcohol consumption
- Physical inactivity and obesity
- Diabetes
- High cholesterol, and particularly high levels of “bad cholesterol” (LDL)


