
Subarachnoid Hemorrhage (SAH)
Overview
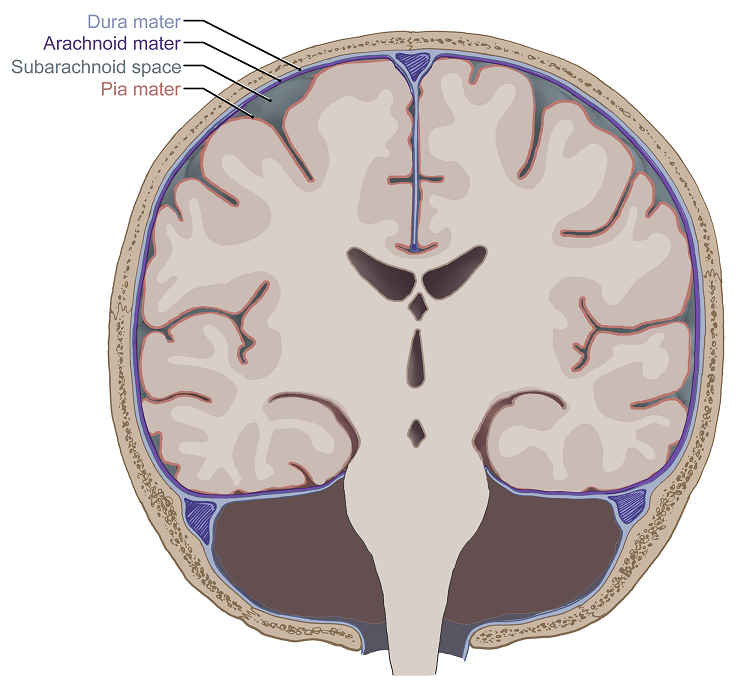
A subarachnoid hemorrhage (SAH) is a type of hemorrhagic stroke caused by bleeding into the subarachnoid space, which is the area between the brain and the thin tissues, called meninges, that cover it.
The subarachnoid space contains cerebrospinal fluid (CSF), which cushions and protects the brain and major blood vessels. When bleeding occurs here, it can cause significant irritation, increased pressure, and disruption of normal brain function.
When to call 9-1-1: A subarachnoid hemorrhage is life-threatening and warrants immediate medical attention.
If you or someone around you experience the sudden onset of a ‘thunderclap headache’ (often described as the worst headache of your life), paralysis of the face or other body parts, nausea and vomiting, or light sensitivity (photophobia), call 9-1-1 and wait for help to arrive.
What causes a subarachnoid hemorrhage?
The most common cause of a subarachnoid hemorrhage (SAH) is the rupture of a cerebral aneurysm—a weak spot in the wall of a blood vessel that balloons out and bursts. These weak spots develop over time due to personal risk factors like high blood pressure, smoking, genetic predisposition, and connective tissue disorders that weaken arterial walls and, in turn, encourage aneurysms to form.

Head injuries from falls, vehicle accidents, or other trauma can cause blood vessels to tear from impact, leading to bleeding in the subarachnoid space.
Although less common, arteriovenous malformations (AVMs) can bleed into the subarachnoid space. AVMs are abnormal tangles of blood vessels that create direct connections between arteries and veins, bypassing the normal capillary network. And because high-pressure blood flows into these connections, AVMs are prone to rupture, which can lead to a subarachnoid hemorrhage.
Bacteria or other pathogens can also weaken arterial walls, forming aneurysms that are vulnerable to rupture. These are known as mycotic aneurysms, which develop from an infection. Although less common, mycotic aneurysms can be considered a cause of SAH, especially in those with a history of systemic infection.
Other causes of SAH include the use of certain drugs, like cocaine, which causes sudden spikes in blood pressure and increases the risk of an aneurysm rupturing. Abnormal clotting conditions can also contribute to bleeding risks, although they more commonly affect other types of intracranial hemorrhage.

Subarachnoid Hemorrhage (SAH) Symptoms
The main symptom of subarachnoid hemorrhage is a sudden and severe headache, also known as a “thunderclap” headache. It’s often described as the worst headache of a person’s life and reaches peak intensity within seconds to minutes.
Most subarachnoid hemorrhage symptoms come on suddenly, meaning you or someone you know might experience any of the following:
- Neck stiffness and pain: Blood in your subarachnoid space can irritate the brain’s protective layers, leading to neck stiffness. Even slight neck movements may cause discomfort.
- Light sensitivity: Bright lights can exacerbate your headache or cause additional discomfort.
- Nausea and vomiting: The sudden rise in intracranial pressure and irritation of the brain can trigger nausea and severe vomiting.
- Focal symptoms: Weakness, numbness, or difficulty with speech, balance, or coordination may occur, depending on the extent of the hemorrhage.
- Cognitive changes: Difficulty concentrating, slowed responses, or struggles with memory can occur. Disorientation or confusion shortly after a hemorrhage is also common.
- Seizures: Seizures can develop due to the irritation of and damage to your brain tissue during a subarachnoid hemorrhage.
- Visual disturbances: If the bleed affects areas of the brain involved in vision, you may experience problems like double vision, vision loss, eyelid drooping, and uneven pupil size.
- Decreased consciousness or loss of consciousness: In more severe cases, you may briefly lose consciousness or even enter a coma.
If you’re experiencing symptoms of subarachnoid hemorrhage, call 9-1-1 immediately.
A subarachnoid hemorrhage is a critical condition that requires urgent medical attention. Without emergency medical treatment, subarachnoid hemorrhage can result in permanent brain damage or death.

Recognizing a stroke quickly and calling 9-1-1 leads to faster diagnosis, treatment, and better recovery. People should “BE FAST” when it comes to stroke.
Here’s how to BE FAST:
- B – BALANCE: Ask the person to walk. Do they have trouble keeping their balance or walking normally?
- E – EYES: Ask the person about their eyesight. Have they lost vision or experienced vision changes in one or both eyes?
- F – FACE: Ask the person to smile. Does one side of the face droop?
- A – ARMS: Ask the person to raise both arms. Does one arm drift downward?
- S – SPEECH: Ask the person to repeat a simple phrase. Is their speech slurred or strange?
- T – TIME: If you observe any of these signs, call 9-1-1 immediately.
Subarachnoid Hemorrhage (SAH) Diagnosis
It’s critical to diagnose a subarachnoid hemorrhage as soon as possible—the rapid onset and intensity of symptoms are essential clues, and a prompt evaluation is necessary. This is because the effectiveness of certain diagnostic tests depends on how soon they’re performed after hemorrhaging.
Brain imaging should be done immediately upon arrival at the hospital or curbside in a mobile stroke unit if it’s available for a definitive diagnosis.
If you’re experiencing any of the symptoms of a subarachnoid hemorrhage, doctors may use the following tests to reach a diagnosis quickly:
- Physical and neurological exam: Your healthcare provider will ask about your symptoms, overall health, and family history of stroke or related conditions. Next, they’ll complete a neurological examination to assess your neurological function, including reflexes, coordination, strength, and sensation.
- Cerebral angiography: The gold standard for detecting vascular lesions, cerebral angiography uses a special dye and X-rays to take detailed images of the blood vessels in the brain. A thin tube is inserted into an artery, usually in the leg, and guided up to the brain to deliver the dye. This allows doctors to see issues like a burst blood vessel, aneurysm, or abnormal vessel formation. It’s invaluable in diagnosing the cause of a hemorrhagic stroke and planning the best treatment.
- Electrocardiogram (ECG): An electrocardiogram is a simple and timely test that records electrical signals in the heart and can detect irregular heart rhythms.
- Echocardiogram: Also known as an “echo,” an echocardiogram is a non-invasive imaging test that uses ultrasound waves to create detailed pictures of the heart and its structure, function, and movement.
- Cerebrovascular testing: This group of testing describes the various tools used to diagnose conditions affecting the blood vessels inside and around the brain.
- Blood tests: These include a complete blood count (CBC) to check for infection, clotting issues, or anemia; coagulation tests to assess blood clotting ability; glucose levels to rule out hypoglycemia; lipid panels to check cholesterol; and markers for infectious or clotting disorders.
- Lumbar puncture: Also known as a spinal tap, a lumbar puncture is not routinely used to diagnose a stroke but may be done in specific cases where additional information is needed to clarify the diagnosis—particularly when there’s suspicion of a subarachnoid hemorrhage or another condition mimicking stroke. A lumbar puncture involves a needle being inserted into the lower part of the spinal canal to collect cerebrospinal fluid (CSF) for analysis.
Our team at Barrow Neurological Institute’s Petznick Stroke Center can perform a full range of diagnostic tests to determine the exact cause of a stroke, including a subarachnoid hemorrhage, 24 hours a day, seven days a week.


Subarachnoid Hemorrhage (SAH) Treatment
The choice between treatment options for a subarachnoid hemorrhage (SAH) depends on multiple factors, like the cause of the bleed, its location, and your overall health. A multidisciplinary team of neurosurgeons, interventional neuroradiologists, and critical care specialists typically collaborates to determine the best approach for each case.
Surgical Treatments
Surgical treatments for a subarachnoid hemorrhage focus on securing the source of bleeding—most often a ruptured aneurysm—to prevent rebleeding and further complications. Depending on the cause of the bleed, treatment may involve:
- Microsurgical clipping: In this procedure, a neurosurgeon surgically opens the skull to access the brain—known as a craniotomy—and then uses specialized tools to isolate the ruptured aneurysm. A small metal clip is placed around the neck of the aneurysm, effectively sealing it off from the blood circulation. When an aneurysm is in an accessible location, this procedure is often the preferred approach.
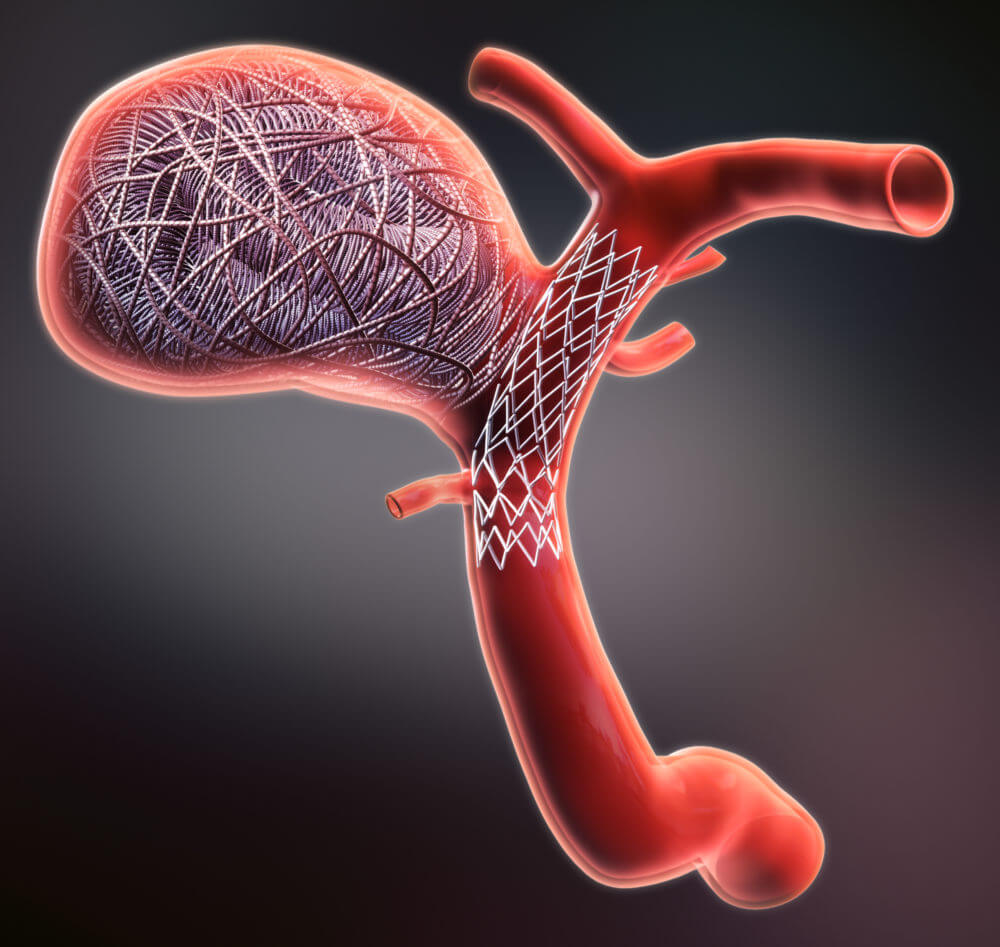
- Endovascular surgery: Although it’s not open surgery in the traditional sense, endovascular surgery, or “coiling,” is a minimally invasive surgical treatment. In this procedure, a catheter is inserted through a blood vessel—usually in the groin—and guided to the brain aneurysm. Tiny coils are then released into the aneurysm, which promotes clotting and eventually seals off the aneurysm from circulation.
- Ventricular drainage: If SAH leads to hydrocephalus, doctors may place an external ventricular drain to drain excess cerebrospinal fluid (CSF) and relieve pressure within the skull.
- Decompressive craniectomy: In rare cases where there’s significant brain swelling or increased intracranial pressure that doctors can’t manage through other measures, they may temporarily remove part of the skull to allow the brain to swell safely. During a depressive craniotomy, a neurosurgeon will make an incision in the scalp and temporarily remove a portion of the skull using intraoperative imaging and specialized tools.

Nonsurgical Treatments
Nonsurgical treatment options focus on stabilization, symptom management, and preventing complications. These approaches can include:
- Blood pressure management: Regulating blood pressure helps prevent hemorrhage rebleeding, meaning medications to lower or stabilize blood pressure are often an essential part of treatment.
- Vasospasm prevention: The blood in the subarachnoid space can irritate arteries, causing them to constrict, which leads to reduced blood flow and further brain injury. Nimodipine, a calcium channel blocker, is often used to minimize risk.
- Anti-seizure medications: If a subarachnoid hemorrhage causes seizures or there’s a high risk of seizures, your doctor will prescribe anti-seizure medications.
- Supportive care: This includes pain control, anti-nausea medications, electrolyte and fluid balance, and close monitoring.
If the underlying cause of a subarachnoid hemorrhage is not promptly treated, there’s a risk of rebleeding. Additionally, blood in the cerebrospinal fluid (CSF) can interfere with CSF circulation, leading to fluid buildup and increased intracranial pressure, known as hydrocephalus.
People can recover with minimal side effects or deficits after receiving treatment for a subarachnoid hemorrhage—especially if the hemorrhage was small and quickly treated. However, others can experience lasting cognitive and physical challenges.
One Central Location with Multiple Treatment Options
At the Petznick Stroke Center at Barrow Neurological Institute, we’re dedicated to best-in-class stroke care and exhaustive research to find new ways to treat and prevent stroke. In fact, our Center cares for more stroke victims than any other center in the southwestern U.S. We’re also the Southwest’s leading stroke research center; conducting more clinical treatment and prevention research trials than any other institution in the region.
From pre-hospital settings to reintegration into the community after a stroke, the Petznick Stroke Center offers a complete spectrum of care for you or your loved one.
Neuro-Rehabilitation for Quality of Life
Neuro-rehabilitation is key to hemorrhagic stroke and subarachnoid hemorrhage recovery. While it doesn’t reverse brain damage, neuro-rehabilitation can help patients achieve the best long-term outcome possible.
Neuro-rehabilitation treatments will vary, depending on the part of the brain that’s been affected and the severity of the stroke. Treatments can be provided in an acute care hospital, a rehabilitation hospital, or an outpatient setting. At Barrow Neurological Institute, our CARF-accredited Neuro-Rehabilitation Center offers inpatient, outpatient, and transitional rehabilitation programs. We also lead the industry in using neuro-robotics. These cutting-edge technologies allow patients to reach unprecedented heights in function and independence.
Common Questions
How common is subarachnoid hemorrhage?
Subarachnoid hemorrhage (SAH) is relatively rare compared to other types of stroke. The incidence rate for subarachnoid hemorrhage is between 10 to 14 cases per 100,000 people annually in the U.S. This translates to roughly 5% of all stroke cases.
Who experiences a subarachnoid hemorrhage?
Because subarachnoid hemorrhage (SAH) can be the result of a traumatic head injury, it can happen to anyone. However, middle-aged adults between 40 and 60 years old are more commonly affected—particularly women with underlying risk factors like hypertension, smoking, or a family history of aneurysms. A family history of brain aneurysms or SAH will increase the overall risk, and genetic conditions like polycystic kidney disease, Ehlers-Danlos syndrome, or fibromuscular dysplasia (FMD) can predispose individuals to aneurysms.
The spontaneous rupture of an aneurysm, a balloon-like bulge in the wall of a blood vessel, is a frequent cause of subarachnoid hemorrhage. In fact, it’s estimated that 1 in 50 people are living with an aneurysm that has not ruptured. Brain aneurysms are more common in adults than children and slightly more common in women than men.
A less common blood vessel abnormality called an arteriovenous malformation (AVM) can also rupture and cause subarachnoid hemorrhage. AVMs are congenital vascular malformations, meaning they’re present from birth, and are most often diagnosed in people between the ages of 20 and 40.
Lastly, smoking, excessive alcohol consumption, blood thinners, and use of illicit drugs like cocaine or methamphetamine are also associated with increased subarachnoid hemorrhage risk.
What is the prognosis for someone who experiences a subarachnoid hemorrhage?
The prognosis after a subarachnoid hemorrhage (SAH) will depend on the severity of the bleeding, the location of the hemorrhage, the timeliness of treatment, and a person’s age and overall health. Generally speaking, more significant amounts of bleeding or more extensive aneurysm involvement tend to be associated with worse outcomes. Complications like vasospasm—the narrowing of cerebral arteries—or hydrocephalus can worsen the prognosis.
On average, SAH has a high mortality rate, with between 25% and 50% of patients not surviving the initial event or the complications that can follow. Some people make a full recovery from subarachnoid hemorrhage, while others experience long-term neurological or cognitive deficits. These can include:
- Cognitive dysfunction, such as challenges with memory and concentration
- Epilepsy
- Fatigue
- Headaches
- Mood disorders, such as depression and anxiety
- Speech and language deficits
- Vision problems
- Paralysis
Can a subarachnoid hemorrhage be prevented?
While not all subarachnoid hemorrhages (SAHs) are preventable—especially those caused by congenital conditions—some steps can help reduce your risk:
- Blood pressure management: High blood pressure can stress vessel walls, so keeping it under control is crucial.
- Avoiding tobacco: Smoking damages blood vessels and increases the risk of aneurysm formation and rupture.
- Moderating alcohol consumption: Excessive alcohol use can contribute to high blood pressure and vascular damage.
- Safety practices: Wearing seat belts and helmets and taking precautions in other high-risk activities can reduce the likelihood of head traumas that can lead to SAH.
Regular medical check-ups and imaging studies, like CT scans, can help detect aneurysms early in people with a known family history or other genetic predispositions.


