
Thyroid Cancer
Overview
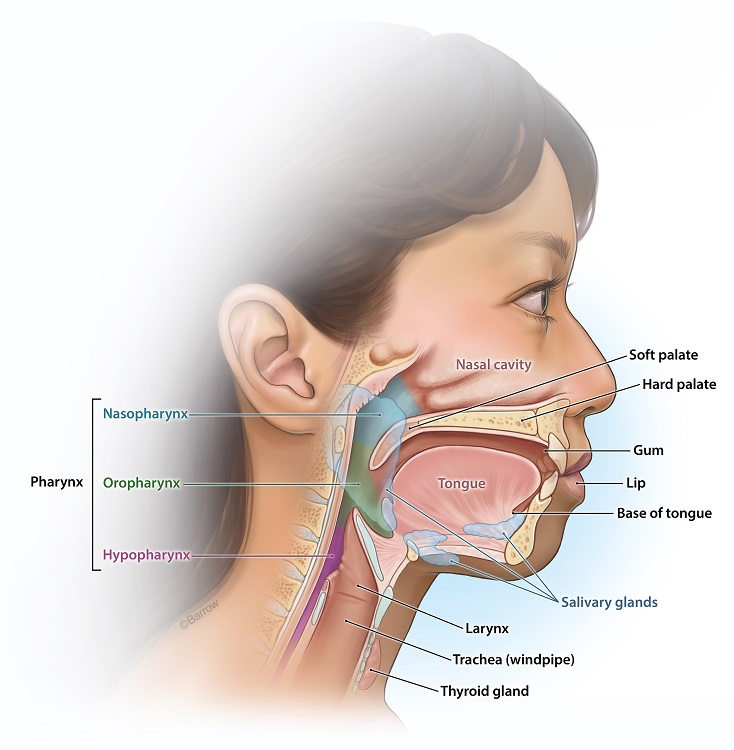
Thyroid cancer is a type of head and neck cancer that starts in the thyroid gland, a small, butterfly-shaped gland in your lower neck, just below the cartilage that protects your voice box. The thyroid is pivotal to your body’s metabolism, helping to regulate heart rate, blood pressure, body temperature, and weight.
Thyroid cancer may not cause any symptoms early in the disease. However, as it grows, it can cause a lump or swelling in your neck, pain radiating from the front of your neck, hoarseness or other voice changes, trouble swallowing or breathing, and a constant cough unrelated to a cold.
The cause of thyroid cancer isn’t always clear, but several factors can increase the risk of developing it, including:
- High radiation exposure, especially during childhood
- A family history of thyroid cancer or genetic conditions that increase the risk
- Being female; women are more likely to develop thyroid cancer than men
- Certain genetic mutations
Physicians diagnose thyroid cancer using a combination of physical exams, blood tests to check thyroid function, imaging tests (like ultrasound), and sometimes a biopsy, where a sample of thyroid tissue is removed and analyzed under a microscope for cancer cells.
Thyroid cancer treatment depends on the type of tumor, its stage, and whether it has spread. Options include surgery to remove some or all of the thyroid gland, radioactive iodine treatment to destroy thyroid cancer cells with minimal impact on the rest of the body, and thyroid hormone therapy to replace the hormones the thyroid would usually make and to help prevent cancer from returning.
Radiation therapy and chemotherapy are less commonly used but may be recommended in certain situations.
The outlook for thyroid cancer is generally good, especially for the more common types that are diagnosed at an early stage. For example, papillary and follicular thyroid cancers have high cure rates with appropriate treatment. Even for more aggressive types, advances in treatment are improving outcomes and quality of life.
It’s essential to have regular follow-ups with your healthcare provider if you’ve been diagnosed with or treated for thyroid cancer, as monitoring is crucial for managing the condition effectively.
Types of Thyroid Cancer
There are several types of thyroid cancer, and they can vary significantly in their aggressiveness. The most common types include:
- Papillary Thyroid Cancer: This is the most common type, making up about 70-80% of all thyroid cancers. It usually grows very slowly and is typically treatable.
- Follicular Thyroid Cancer: The second most common type, accounting for 10-15% of all cases. Follicular tumors usually grow slowly but can spread to other body parts more often than papillary cancer.
- Medullary Thyroid Cancer: Comprising 2-4% of thyroid cancers, medullary thyroid cancer can be more challenging to treat. Genetic syndromes could play a role in causing it.
- Anaplastic Thyroid Cancer: Rare, aggressive, and challenging to treat, anaplastic thyroid cancers account for less than 2% of all thyroid cancers.

Symptoms of Thyroid Cancer
Thyroid cancer often doesn’t cause any symptoms in its early stages. However, as it grows, it can lead to signs and symptoms that you might notice. Some of the symptoms that may be associated with thyroid cancer are below.
- A Lump in the Neck: One of the most common signs is noticing a lump or swelling in your neck. This lump is where the cancer is growing in the thyroid gland. It might not be painful, but you can often see or feel it when you touch the area.
- Changes in Your Voice: The thyroid is near your vocal cords and the nerves that control them, so a growing tumor might press on them and cause your voice to become hoarse or change in some way. Most commonly due to compression or invasion of the recurrent laryngeal nerve, this change in voice is usually persistent and doesn’t go away like it might with a common cold.
- Difficulty Swallowing or Breathing: As the lump gets bigger, it can press against your windpipe or esophagus (the tube that connects your mouth and stomach), making it harder to swallow or breathe, especially when lying down or at night.
- Pain in the Neck: You might feel pain in the front of your neck near the thyroid. Sometimes, this pain can extend up to your ears.
- A Constant Cough: If you have a cough that isn’t related to a cold or allergy and doesn’t go away, it could be a sign of thyroid cancer, especially if other symptoms accompany it.
Conditions other than cancer can cause these symptoms, like an infection or benign thyroid nodules. However, if you notice any of these symptoms, especially if they persist or worsen, it’s a good idea to visit a doctor. They can perform tests to find out what’s causing them and provide you with the appropriate care.
Treatments for Thyroid Cancer
Treating thyroid cancer involves a few different strategies, depending on the type and stage of the cancer, as well as your overall health.
Surgery
Thyroid cancer surgery is a routine and effective treatment for removing thyroid cancer. The goal of the surgery is to take out the cancerous part of the thyroid gland or, in some cases, the entire gland itself. Surgery for thyroid cancer falls under three broad categories:
- Lobectomy: This involves removing one lobe (half) of the thyroid. If the cancer is small and confined to one lobe, this may cure the disease. The advantage is that it might leave you with some thyroid function, possibly reducing the need for lifelong thyroid hormone replacement.
- Total Thyroidectomy: This surgery removes all of the thyroid gland. It’s more common, especially if the cancer is found in both lobes, is more extensive, or there’s a risk it might spread. After this surgery, you will need thyroid hormone replacement therapy to substitute the gland’s functions for the rest of your life.
- Lymph Node Removal: If there’s a concern that the cancer has spread to nearby lymph nodes, your surgeon may also remove some of these nodes during the operation to check for cancer cells.

Surgery
Before undergoing surgery for head and neck cancer, you’ll talk with your surgeon about the procedure, including what to expect and any risks involved. You may undergo several tests, such as blood tests and imaging scans, to help plan the surgery. Your medical team will also discuss how to prepare for the operation, including any medication changes.
Surgery usually takes a few hours and is done under general anesthesia, which means you’ll be asleep and won’t feel pain during the procedure. The surgeon makes an incision at the base of your neck to access the thyroid. The incision usually falls in a natural crease of the skin, making the scar less noticeable after it heals.
After surgery, you may spend a short time in the hospital to recover. It’s common to experience some pain, hoarseness, or difficulty swallowing temporarily, but these symptoms typically improve as you heal. Your medical team will monitor your calcium levels since the surgery can sometimes affect the parathyroid glands, which regulate calcium.
If your entire thyroid is removed, you’ll need to take thyroid hormone replacement medication to perform the functions your thyroid used to. This medication helps regulate your body’s energy and metabolism. Your doctor will work with you to find the proper dosage.
Thyroid cancer surgery aims to remove all of the cancer and minimize the risk of it coming back while also preserving as much of your normal thyroid function as possible and avoiding complications. With careful planning and follow-up care, most people can expect to live normal, healthy lives after surgery.
Radioactive Iodine Treatment
After surgery, especially if your whole thyroid is removed, you might undergo radioactive iodine treatment. This involves swallowing a therapeutic dose of radioactive iodine (iodine-131), which travels through your blood and kills any remaining thyroid cells, including cancer cells. This treatment helps to reduce the chance of cancer returning.
Thyroid Hormone Therapy
Since your body needs thyroid hormones to function correctly, and your thyroid might be removed or no longer working well, you’ll likely need to take thyroid hormone pills. These pills replace the hormones your thyroid would usually make. They also have the added benefit of helping to stop any remaining cancer cells from growing.
External Radiation Therapy and Chemotherapy
Radiation therapy is less common for thyroid cancer. Still, it can be used in some cases, primarily if the cancer has spread to other parts of your body and surgery isn’t possible. It involves targeting high-energy rays at the tumor to kill the cancer cells.
Chemotherapy, which is the use of drugs to kill cancer cells, is rarely used for thyroid cancer. It might be considered if the tumor is very aggressive and not responding to other treatments.
Targeted Therapy
Your doctor might suggest Targeted therapy if your tumor doesn’t respond to radioactive iodine treatment. These drugs specifically target abnormalities within cancer cells to stop them from growing.
What to Expect
Regular follow-up appointments are crucial after treatment for thyroid cancer. Your doctor will monitor your condition, check for signs of cancer returning, and adjust your thyroid hormone dosage as needed.
You will need to take thyroid hormone pills for the rest of your life if the bland has been removed entirely. With the correct dosage, you can live a normal, healthy life.
The main goal of treating thyroid cancer is to remove the cancer, prevent its return, and maintain your quality of life. With early detection and proper treatment, the prognosis for thyroid cancer is often excellent, with many patients living long and healthy lives after treatment.
Staging of Thyroid Cancer
The stages of thyroid cancer help doctors understand how far the cancer has progressed and guide them in determining the best treatment options. Staging can vary a bit depending on the specific type of thyroid cancer, but for the most common (differentiated) thyroid cancers it is classified as follows:
Stage I
- For patients under 55: All cancers are considered Stage I unless they have spread to distant sites.
- For patients 55 and older: The tumor is limited to the thyroid and is less than 4 cm in size.
Stage II
- For patients under 55: Any cancer that has spread to distant sites.
- For patients 55 and older: Tumors between 2 and 4 cm that are limited to the thyroid that have spread to nearby lymph nodes, or:
- Tumors greater than 4 cm that are limited to the thyroid gland or those that are only minimally growing beyond the thyroid with or without spread to nearby lymph nodes.
Stage III
- Only for patients 55 years and older, this stage indicates a tumor of any size that has spread grossly beyond the gland to nearby structures with or without any spread to the lymph nodes.
Stage IV
- Only For patients 55 and older it describes the following:
- Any tumor that has grown beyond the thyroid gland to involve nearby critical structures such as the tissue protecting the spine, carotid artery, or large blood vessels within the chest.
- Any cancer that has spread to distant sites, such as bones, abdominal organs, or other body parts.
Staging is crucial for estimating your prognosis and the best treatment approach. Early-stage cancers generally have a better prognosis and may require less aggressive treatment. Advanced-stage cancers might need a combination of treatments, such as surgery, radioactive iodine therapy, external radiation therapy, or targeted therapy.
It’s important to note that thyroid cancer, especially in its early stages, often has an excellent prognosis. Advances in treatment have significantly improved outcomes, even for more advanced cancers.
Common Questions
What is the survival rate for thyroid cancer?
The survival rate for thyroid cancer is generally very favorable. It’s one of the most treatable forms of cancer, especially when diagnosed early. Survival rates can vary based on several factors, including the type of thyroid cancer, its stage at diagnosis, your age, and you overall health. Here’s a general overview of the five-year relative survival rates based on the most common type of thyroid cancer, papillary thyroid cancer, which accounts for the majority of cases:
- Localized (cancer is confined to the thyroid): Nearly 100%. This means that almost all people diagnosed with cancer that hasn’t spread outside the thyroid can expect to live at least five years after diagnosis.
- Regional (cancer has spread to nearby tissues or lymph nodes): Also near 100%. People whose cancer has spread locally still have an excellent prognosis.
- Distant (cancer has spread to other parts of the body): The survival rate is lower but still relatively high compared to many other cancers, at around 78%. However, this rate can vary depending on the specifics of the spread and the subtype of thyroid cancer.
The survival rates can differ among the various types of thyroid cancer:
- Papillary and Follicular: These types have the highest survival rates, with most patients experiencing excellent outcomes.
- Medullary: This type has a somewhat lower survival rate than papillary and follicular but is still considered treatable, especially if caught early.
- Anaplastic: This is a rare and aggressive form of thyroid cancer with a lower survival rate. However, it accounts for a tiny percentage of thyroid cancer cases.
Other factors can affect survival:
- Age: Younger people generally have a better prognosis.
- Tumor Size and Spread: Smaller tumors confined to the thyroid gland have a better prognosis.
- Response to Treatment: People who respond well to treatment, including those with cancers sensitive to radioactive iodine, often have a better outcome.
It’s important to remember that statistics are based on large groups of people and can’t predict outcomes for any individual. Advances in treatment and early detection have improved survival rates over time. Additionally, many people with thyroid cancer not only have a good prognosis in terms of survival but also maintain a good quality of life after treatment.
If you or someone you know has been diagnosed with thyroid cancer, it’s crucial to discuss the prognosis with a healthcare provider, as they can provide information tailored to the individual’s specific situation.
How common is thyroid cancer?
Thyroid cancer is considered a relatively common type of cancer, especially among certain demographics. However, it’s important to note that compared to other cancers, the prognosis for thyroid cancer is often very favorable, with high survival rates.
Thyroid cancer has been on the rise in many countries over the past few decades. This increase is partly attributed to the improved detection of small thyroid cancers through advanced imaging technologies.
Thyroid cancer is more common in women than in men. The reasons for this difference are unclear but may involve hormonal, genetic, and environmental factors.
Thyroid cancer can occur at any age but is most frequently diagnosed in people 20 to 55.
Papillary thyroid cancer, the most common type, accounts for about 70-80% of all cases and has the best prognosis.
Despite its relatively high incidence, the overall 5-year survival rate for thyroid cancer is about 98%, making it one of the most treatable forms of cancer. Early detection and treatment significantly contribute to positive outcomes.
Resources



References
- Moustafa Mourad, Thomas Jetmore, Ameya A. Jategaonkar, Sami Moubayed, Erin Moshier, Mark L. Urken, Epidemiological Trends of Head and Neck Cancer in the United States: A SEER Population Study, J Oral Maxillofac Surg. 2017 Dec;75(12):2562-2572. doi: 10.1016/j.joms.2017.05.008. Epub 2017 May 22. PMID: 28618252.
- American Cancer Society. Thyroid Cancer. March 28, 2024.