Clinical Images: Postpenetrating Trauma Cerebrospinal Fluid Fistula
Authors
John F. Hamilton, MD
A. Giancarlo Vishteh, MD
William L. White, MD
Division of Neurological Surgery, Barrow Neurological Institute, Mercy Healthcare Arizona, Phoenix, Arizona
Key Words : cerebrospinal fluid fistula, penetrating trauma
A 43-year-old male presented to an outside facility after sustaining a deep puncture/stab wound to the left nostril. The small stab laceration was closed primarily, and the patient was discharged. He presented to our institution 2 days later complaining of persistent headaches and intermittent rhinorrhea. On examination he was afebrile, neurologically intact, and without nuchal rigidity or photophobia. A sutured laceration was present at the verge of the left nostril. He exhibited cerebrospinal fluid rhinorrhea (positive glucose dipstick) on the “reservoir test.”
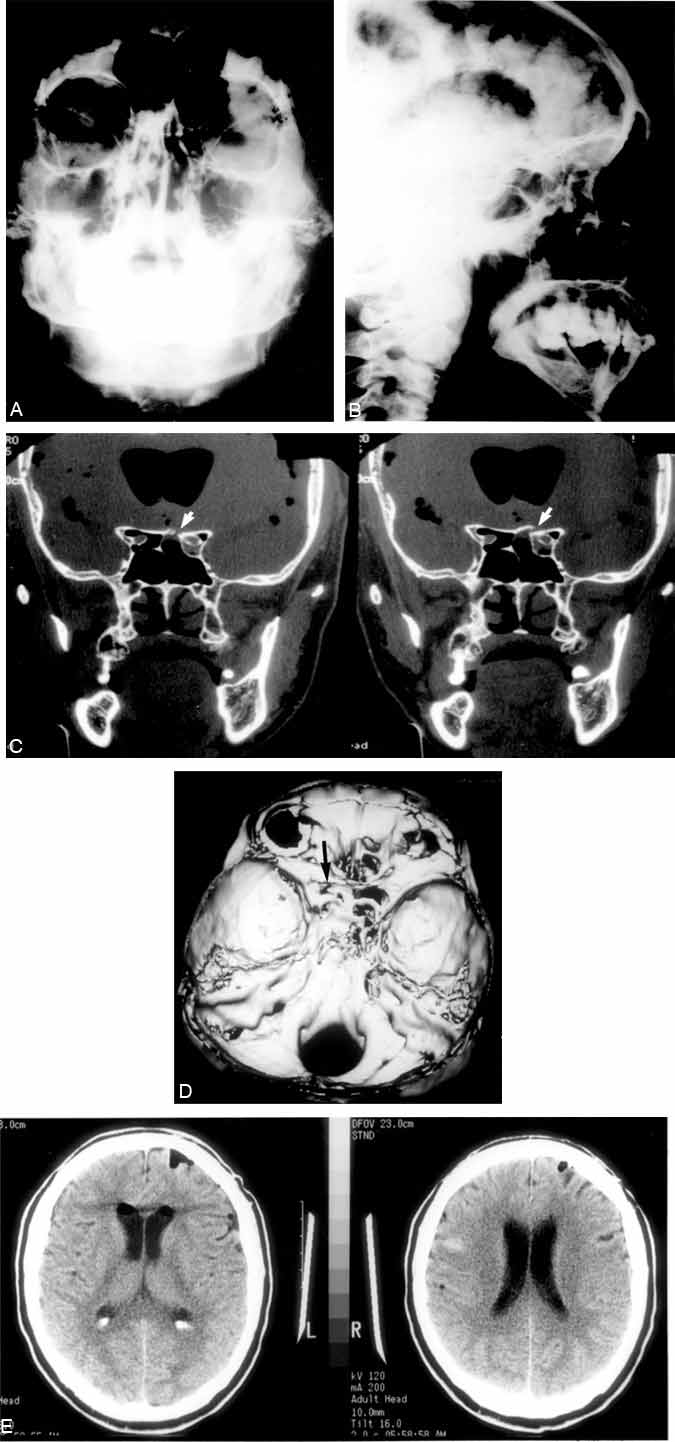
Anteroposterior (Panel A) and lateral (Panel B) radiographs of the skull demonstrated massive intraventricular pneumocephaly. Coronal computed tomography (CT) (Panel C) revealed a fracture (arrows) of the left paramedian sphenoid bone and the presence of intraventricular air. The fracture is also shown on a three-dimensional CT reconstruction (arrow) (Panel D). He underwent a successful transsphenoidal packing and repair of his fistula and was discharged 3 days later. Postoperative CT (Panel E) demonstrated almost complete resolution of the pneumocephaly.