
A Nursing Perspective of Gamma Knife Treatment
Carol M. Browner, RN
Karl Hendrickson, MD†
Gamma Knife Center and †Division of Neuroanesthesiology, Barrow Neurological Institute, Mercy Healthcare Arizona, Phoenix, Arizona
Abstract
The role of the registered nurse is pivotal to the successful operation of a Gamma Knife Unit. The technology is still relatively new and available at a limited number of sites. This article therefore describes the clinical pathway of a patient undergoing Gamma Knife treatment, focusing on the role of the registered nurse in the patient’s care.
Key Words : Gamma Knife, nursing, stereotactic radiation
Use of the Gamma Knife is still relatively new in North America. The first unit was installed at the University of Pittsburgh in August 1987. Today 25 units are operational in the United States, with a total of 75 worldwide. In preparing for the inception of a Gamma Knife Unit at the Barrow Neurological Institute, the nurse coordinator visited several other units in the United States. The nurses’ roles at these sites were observed, and it became evident that nursing plays a pivotal role in the inception, operation, and success of these radiosurgical endeavors. The role of the nurse coordinator for the new unit was then designed to fit the needs of our institution. This article reviews the clinical pathway of the patient undergoing Gamma Knife treatment, emphasizing the role of this nurse coordinator.

Most patients referred for Gamma Knife treatment are victims of a brain tumor or are afflicted with an arteriovenous malformation (AVM). At our institution, patients with a brain tumor are referred for treatment by the BNI Tumor Board. The Tumor Board, comprised of a group of physician experts, meets weekly to discuss treatment options for such patients. The board includes neuro-oncologists, oncologists, neurologists, neurosurgeons, neuroradiologists, neuropathologists, and radiation oncologists. The attending physician, who may be from any of these disciplines, may also participate in this process. Once the decision is made to use the Gamma Knife for treatment, the case is referred to the Gamma Knife Stereotactic Radiosurgery Committee where it is reviewed for appropriateness. The Stereotactic Committee is comprised of the authorized users of the Gamma Knife and includes a neurosurgeon, a radiation oncologist, a physicist, and a nurse. Patients referred for obliteration of an AVM also must be reviewed by the Stereotactic Committee.
The attending physician discusses treatment alternatives with the patient. If the patient selects Gamma Knife treatment, the nurse coordinator, assisted by the secretarial support staff, implements the next phase of care. The patient is telephoned and a tentative date and alternative dates for treatment are selected. The admission and treatment date must be coordinated with the availability of the magnetic resonance (MR) imaging, computed tomography (CT) and/or angiography suites as well as with the neurosurgeon and radiation oncologist and, possibly, with an anesthesiologist. During the initial telephone interview, pertinent information is obtained such as third-party payor authorization and a brief medical history, which includes allergies, current medications, and contraindications for MR imaging. The nurse begins a pretreatment checklist that is followed closely until all objectives are met. Pre-authorization must be confirmed before the patient’s admission. Because this process can be slow, careful planning is essential. The pre-authorization number as well as the person’s name from the insurance company who rendered the number must be entered onto the checklist to avoid later confusion. The authorization should include a one-night hospital stay, which the patient usually requires for treatment and observation.
A few days before treatment, the patient tours the facility to become familiar with the Gamma Knife itself. An educational booklet, which describes treatment, potential side-effects, and home-care instructions, is given to the patient. Any laboratory work, radiographic films, or cardiac work-up needed also may be performed during this visit to avoid delays on the day of admission. A screen to evaluate the patient’s compatibility with MR imaging is filled out to ensure the patient’s safety during scanning. Verbal education for the patient and significant others is completed. All the patient’s questions should be answered satisfactorily before this session is terminated and the informed consent signed.
Early on the morning of treatment, the patient reports to the admitting area of the hospital and is taken to the same-day surgical admissions area, known as Sav-A-Day at our institution. A neurosurgery resident performs a complete history and physical examination of the patient if they have not already been done in the physician’s office before admission. The patient changes into hospital clothes, and a nurse completes a nursing physical assessment and secures an intravenous line to the patient before sending the patient to the Gamma Knife suite by gurney or wheelchair. The Gamma Knife nurse receives the patient, who is then taken to the preparation room for the placement of the head frame.
Frame Placement
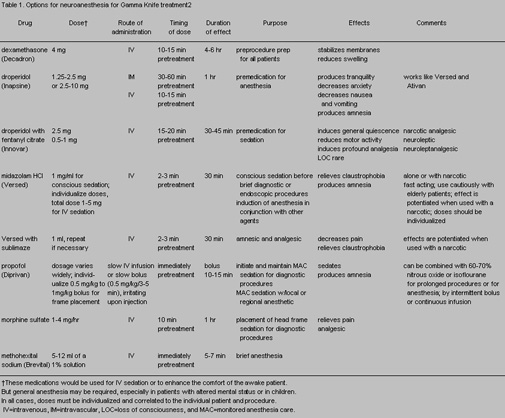
The Leksell stereotactic head frame can be placed with the patient (Fig. 1) under various levels of anesthesia (Table 1). It can be performed with local anesthesia alone or with local anesthesia plus an intravenous medication to reduce pain and stress. A stand-by anesthesiologist may briefly sedate a patient or induce general anesthesia. The patient’s medical condition, age, anxiety level, mental status, and ability to tolerate pain all must be considered when the level of anesthesia is chosen. Medications vary in their ability to sedate and to control pain and are selected depending upon the desired effect. A standard regimen of sedation may not be the best practice to follow when the head frame is applied because patients will differ in their ability to tolerate pain and medication.
Narcan should be available for all patients who receive narcotics. It should be kept in mind that patients are undergoing Gamma Knife treatment for brain disorders, and sedatives and narcotics should be given cautiously to this group because of the potential for depressing the central nervous system and for increasing carbon dioxide, which can increase intracranial pressure. Doses should always be started low, and higher doses can be given according to the patient’s reaction.
Local anesthesia to the pin sites seems best achieved by using a mixture of lidocaine with sodium bicarbonate (9:1). The bicarbonate acts as a buffering agent to reduce the stinging sensation that the lidocaine causes. This mixture appears to affect profoundly a patient’s ability to tolerate pin placement and pressure. Some physicians prefer to use bupivicaine; however, it is incompatible with sodium bicarbonate. A 22- or 25-gauge needle should be used for the skin injection. The nurse prepares the patient’s scalp, usually with an alcohol or an antiseptic scrub, administers medications, and assists with placement of the frame, comforting the patient as necessary.
The patient should be allowed to take his or her critical medications, such as anticonvulsants and cardiac medications, with a sip of water on the morning of treatment. Otherwise, the patient’s oral intake ceases from the midnight before treatment. Pertinent medications should be brought to the Gamma Knife suite and taken as scheduled during treatment if necessary. The patient’s hair should be washed the night before but no creams or hair spray should be applied.
The patient is monitored by pulse oximetry, blood pressure, and electrocardiography. Vital signs are taken before treatment and every few minutes during placement of the frame. Vital signs are then monitored every 30 minutes while the patient is in the Gamma Knife suite and as needed, depending upon the amount of sedation and pain medication administered during the procedure. Oxygen, administered through mask or nasal cannula, is used if necessary. If the patient undergoes general anesthesia, the guidelines for anesthesia monitoring are followed.
Once the head frame is securely in place, the nurse coordinator measures the radii of the patient’s skull by affixing a plastic sphere or bubble to the head frame and recording 24 measurements with the Gamma Knife’s skull scaling instrument. The patient is then transported to the MR imaging, CT, or angiography suites to undergo the three-dimensional imaging necessary for target determination. All three types of imaging require a plastic fiducial box, which is essential for determining the coordinates of the lesion, to be applied to the patient’s head frame. The fiducial box has several grooves, which are filled with liquid contrast material. The grooves appear on radiographic films and are used to calculate the dimensions and position of the targeted lesion.
The nurse is responsible for proper application of these boxes, and an x-ray technologist usually assists with this procedure. Together, the nurse and technologist place the patient on the table. The patient’s head is secured in the proper position on the support base plate or head adaptor, on the couch. A carpenter’s level is used to verify that the patient’s head position is correct. Ear plugs should be supplied to the patient for MR imaging studies. Depending upon the number of tests required, the imaging may last 1 to 3 hours. When the studies are finished, the fiducial boxes should be stored in the Gamma Knife suite rather than in their respective departments to assure that they are not misplaced or broken. The nurse must maintain the boxes and keep their tunnels or grooves filled with liquid contrast media.
After the imaging is completed, the patient is returned to the Gamma Knife suite to rest and to visit with significant others in the holding room. The patient may listen to a tape or compact disc or watch a movie for relaxation. During this time, the physicist and physicians enter the imaging data into the computerized treatment planning system to determine the distribution of the radiation dose, plugging patterns, and shot times. A patient may need more than one radiation shot, depending upon the target under treatment. Each shot may last from a few to approximately 30 minutes. The actual duration of the Gamma Knife treatment varies greatly from one patient to the next. At some point during the treatment planning, the patient is placed on the operating couch temporarily to determine the most appropriate and comfortable gamma angle for his or her treatment. Afterwards, the patient is returned to the holding room until the treatment has been planned completely. The time needed to plan treatment varies from a few minutes to a couple of hours.

Plugging patterns are predetermined by the dose-planning system; however, the flashlight check, performed before each shot of radiation, is a fail-safe method to ensure the patient’s safety. Plugging the ports on the helmet is the nurse’s responsibility. The task can become arduous if many holes must be plugged, especially if more than one helmet is needed during treatment. The four helmets available for use during treatment have ports that range from 4 mm to 18 mm (Fig. 2).
The helmets are changed, as the treatment plan dictates, by the use of a hydraulic lift (Fig. 2) because each helmet weighs more than 400 pounds. The patient is brought into the treatment room on a gurney and helped onto the treatment couch by the nurse and one other person. The patient lies flat and is scooted upward toward the head of the couch (Fig. 3). The stereotactic frame on the patient’s head is aligned with the chosen helmet, which is already secured to the Gamma Knife treatment table. The patient’s head and stereotactic frame are then locked into the helmet.

The patient is left alone, the doors to the room are closed, and treatment begins. The physicist begins the treatment, and the patient and helmet back into the Gamma Knife as the radiation shield is lifted. The patient’s helmet locks into place, aligning itself with the helmet inside the shield. The 201 ports of the inner helmet line up with those of the patient’s helmet, and the radiation is allowed through. Each of the 201 portholes converge the radiation beam onto the same point within the patient’s brain.
The patient remains in this position, unable to move his or her head until the treatment is completed. The patient may listen to music during this time and is encouraged to bring a personal selection of compact discs or cassette tapes. As stated, the duration of the treatment varies and more than one shot may be necessary. If needed, the patient may walk to the bathroom between shots. For each new shot, the coordinates and eye ports are again checked for accuracy. The patient may be in the treatment room for as long as 2 hours, depending upon the treatment plan and the number of shots prescribed.
After treatment, the patient is returned to the preparation room where the frame pins are removed. A battery-powered drill is used to back the pins out of the skull. The drill removes the pins quickly, reducing the pain experienced by the patient. The pin sites are covered with an antimicrobial agent and a gauze pad. The patient is then transported to the assigned hospital room and a report is given to the unit nurse. Patients who receive general anesthesia are transferred to the recovery room before they are admitted to the nursing unit.
Posttreatment Care
After treatment, the patient is given dexamethasone (4 mg) by mouth every 6 hours for 24 hours. While taking the dexamethasone, the patient also takes an H2 antagonist or an antacid every 6 hours. The patient can continue taking any preoperative medications that were prescribed along with any of his or her regular medications. An anti-emetic, a mild analgesic, or an anticonvulsant can be taken as needed.
The patient’s vital and neurological signs should be checked every 2 hours for the first 8 hours and then every 4 hours thereafter. Intravenous solutions should be run at the appropriate rate until the patient can tolerate fluids by mouth. Then the patient is switched to a saline lock and the diet is advanced as tolerated.
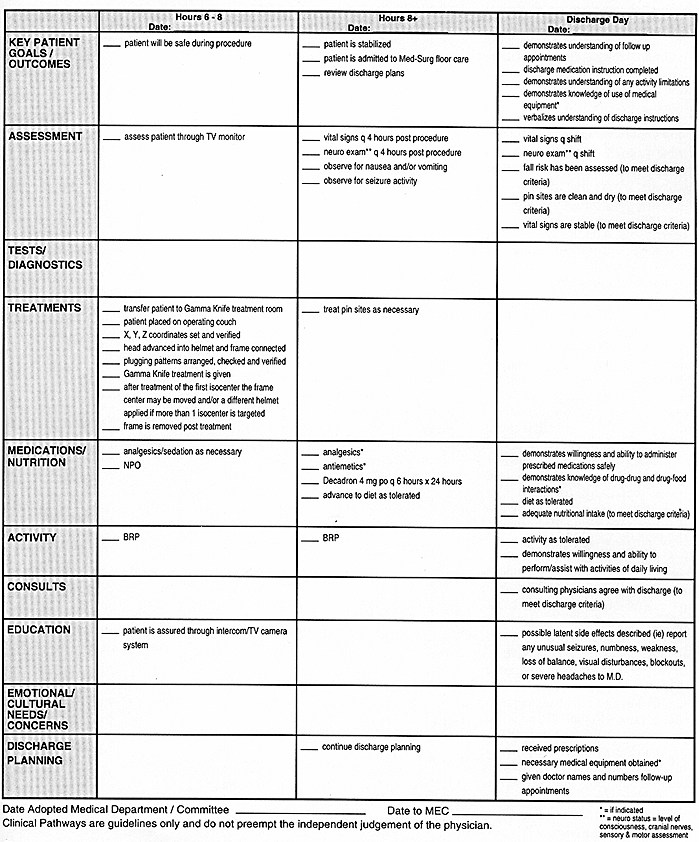
The patient also may be out of bed as tolerated. Routine pin care is instituted and discharge planning continues (Fig. 4).
The patient is discharged the next morning as long as any complications have been stabilized. Immediate complications from the treatment itself are rare. The patient, however, may experience a headache, mainly from the stereotactic frame, nausea or vomiting, or seizures. Complication rates will differ depending upon the diagnosis, but neurological deficits are reported in approximately 3% of all patients.1 The patient is informed to be aware of latent side effects, such as unusual numbness, tingling, weakness, loss of balance, visual disturbances, blackouts, or severe headache. Latent side effects and their rate of occurrence vary from patient to patient, depending upon the diagnosis and location of the lesion. If he or she experiences any of these symptoms, the patient is asked to inform the attending physician.
The patient is given the phone numbers of the appropriate physicians for follow-up appointments. AVMs may close gradually over a couple of years, and the most accurate test for a residual AVM is angiography. Likewise, it may take months before a brain tumor shrinks or is obliterated. Because radiosurgery does not immediately affect the lesions, follow-up examinations and radiographs are imperative. Each patient should be followed for at least 5 years after treatment.
The Role of the Nurse Coordinator
The Gamma Knife nurse is the principal researcher and statistician and must ensure that good records are kept, appropriate follow-up examinations are scheduled for patients, and data are entered into the database in a timely fashion. For each type of lesion, the nurse closely follows a protocol that delineates predetermined dates for follow-up angiography, CT, and MR imaging. The patient and significant others are given a schedule and asked to maintain contact with the attending physician. The nurse, however, is responsible for contacting the patient when the time of the scheduled examination draws near. The nurse, as well as the physicist, acts as a resource for the institution, answering telephone and written queries about Gamma Knife treatment.
Together, the nurse and physicist are responsible for the department’s safety program and quality assurance protocols. The nurse ensures that the Gamma Knife equipment is kept in excellent working condition and that quality assurance protocols and testing procedures are adhered to closely. Radiation safety training is provided annually for all Gamma Knife personnel, and radiation badges are analyzed monthly. Both the physicist and nurse are members of the Hospital Radiation and Safety Committee and advise the hospital’s Radiation Safety Officer of activities within the department. Policies are reviewed annually and revised as needed.
The Gamma Knife nurse serves as a catalyst for the department’s pursuits and coordinates the complicated interdepartmental activities involved in the patient’s radiosurgical treatment. The functions of this challenging role are varied and include being involved with the actual organization and inception of the unit, acting as administrator, delivering patient care, educating patients and family, and participating in research studies. Working with a Gamma Knife project is a relatively new and unique opportunity for the registered nurse who can experience the best of both worlds: working with the technology of the computer age while maintaining personal contact with patients and their significant others.
Acknowledgments
The authors thank the Gamma Knife registered nurses who so willingly shared their knowledge and experiences: Corinne Cloughen, RN, Rocky Mountain Gamma Knife Center, Denver, CO; Aiko Teragowa, RN, MS, The Hospital of the Good Samaritan, Los Angeles, CA; and Mark Wargo, RN, BSN, and Jonet Vacsulka, RN, BSN, University of Pittsburgh Medical Center, Pittsburgh, PA.
References
- Coffey RJ: Stereotactic radiosurgery: Principles, techniques, and instrumentation using the Gamma Knife. Contemp Neurosurg 16(4):1-6, 1994
- Drug Facts and Comparisons: Central Nervous System. Philadelphia: J.B. Lippincott, Wolters Kluwer, pp. 1427-1470.
Suggested Readings
- Ganz JC, Backlund EO, Thorsen FA: The effects of Gamma Knife surgery of pituitary adenomas in tumor growth and endocrinopathies. Stereotact Funct Neurosurg 61(Suppl 1):30-37, 1993
- Kihlström L, Karlsson B, Lindquist C: Gamma Knife surgery for cerebral metastases. Implications for survival based on 16 years experience. Stereotact Funct Neurosurg 61(Suppl 1):45-50, 1993
- Kondziolka D, Lunsford LD, Flickinger JC: Current concepts in Gamma Knife radiosurgery. Neurosurgery Quarterly 3(4):253-271, 1993
- Leksell DG: Stereotactic radiosurgery: Current status and future trends. Stereotact Funct Neurosurg 61:1-5, 1993
- Lindquist C: Gamma Knife radiosurgery. Semin Radiat Oncol 5(3):197-202, 1995
- Lunsford LD: Stereotactic radiosurgery: At the threshold or at the crossroads? Neurosurgery 32(5):799-804, 1993
- Lunsford LD, Kondziolka D, Flickinger JC, et al: Stereotactic radiosurgery for vascular malformations of the brain. Neurosurgeons 12:173-181, 1993
- Mathis JA, Barr JD, Horton JA, et al: The efficacy of particulate embolization combined with stereotactic radiosurgery for treatment of large arteriovenous malformations of the brain. Am J Neuroradiol 16(2):299-306, 1995
- Ogunrinde OK, Lunsford LD, Flickinger JC, et al: Facial nerve preservation and tumor control after Gamma Knife radiosurgery of unilateral acoustic tumors. Skull Base Surg 4(2):87-92, 1994
- Pollock BE, Lunsford LD, Kondziolka D, et al: Outcome analysis of acoustic neuroma management: A comparison of microsurgery and stereotactic radiosurgery. Neurosurgery 36(1):215-229, 1995
- Speiser BL, Shetter AG: Stereotactic radiosurgery of skull base lesions. BNI Quarterly 8(4):35-41, 1992
- Steiner L, Lindquist C, Cail W, et al: Microsurgery and radiosurgery in brain arteriovenous malformations. J Neurosurg 79(5):647-652, 1993