
Clinical Images: Neurofibromatosis with Meningiomatosis
G. Michael Lemole, Jr., MD
A. Giancarlo Vishteh, MD
Robert F. Spetzler, MD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Key Words: meningiomatosis, neurofibromatosis, multiple meningiomas
A 43-year-old female was followed for presumed neurofibromatosis type II (NF-II). Her initial presentation of hearing loss progressed to bilateral deafness. Neuroimaging studies showed bilateral tumors in the cerebellopontine angle and led to the diagnosis of NF-II. One of the acoustic neuromas was resected. The patient later sought treatment for progressive visual loss (acuity 20/400). She also had bilateral palsies of the abducens and facial nerves.
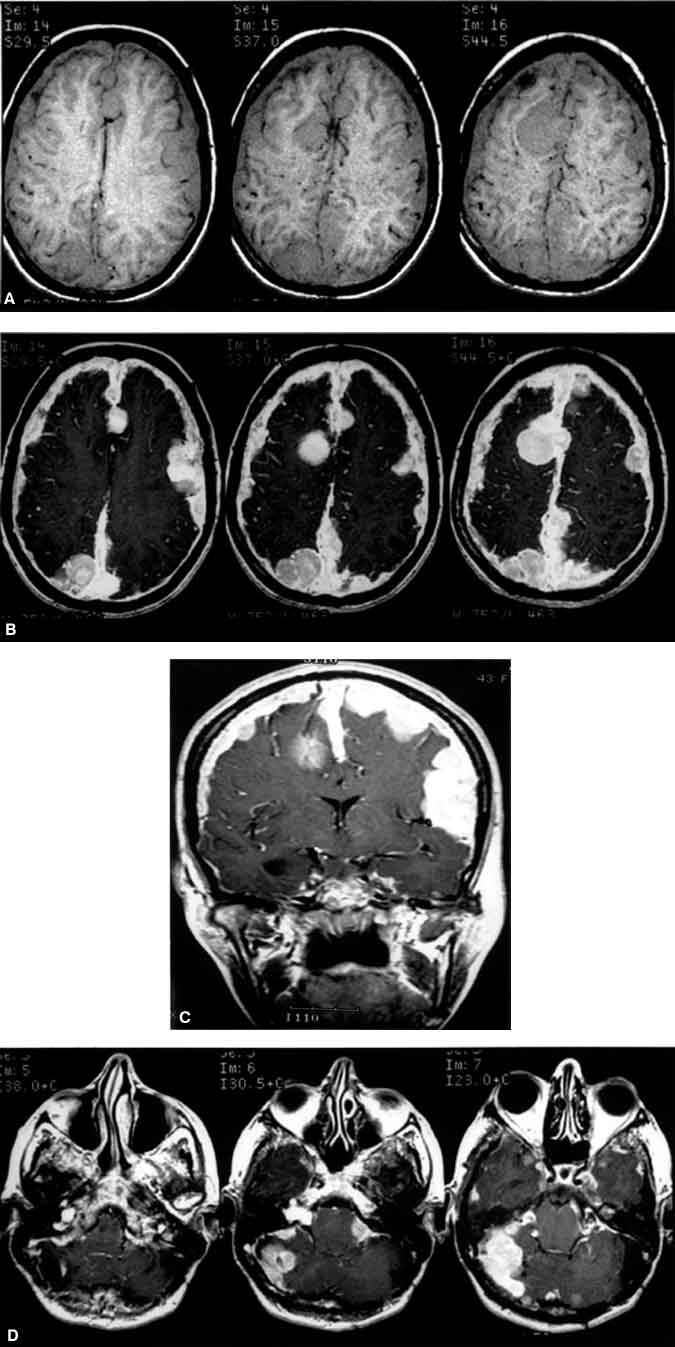
The patient’s most recent magnetic resonance (MR) imaging study demonstrated diffuse meningiomatosis involving the supratentorial compartment and posterior fossa. The tumors brightly enhanced with gadolinium on axial MR images (Panels A and B). Tumor could be seen compressing the optic nerves and interdigitated between the cerebral sulci and fissures (including the Sylvian and interhemispheric fissures) on coronal MR images (Panel C). The resected acoustic neuromas had regrown (Panel D, axial MR images). Because of the diffuse nature of her disease, the patient was managed conservatively. She was placed on steroids and her visual symptoms remained stable.
NF-II belongs to a group of neurocutaneous disorders formerly classified as phacomatoses. This group of disorders is characterized by unique cutaneous manifestations (i.e., café-au-lait spots) and neural tumors and may be associated with dysplasias of other organ systems. Classically, NF-II is characterized by bilateral acoustic neuromas. In their absence, however, NF-II can also be associated with neurofibromas, meningiomas, gliomas, schwannomas, or juvenile cataracts. The locus for the NF-II gene of this inherited disorder (autosomal dominant) is located on chromosome 22.
There is no cure for neurofibromatosis, but surgical intervention is warranted for symptomatic tumors. After an acoustic neuroma has been resected and a patient again becomes symptomatic with an enlarging contralateral tumor that requires surgery, debulking can be considered to save the vestibulocochlear nerve. If radical resection is planned, an auditory brain stem implant can be placed during the same surgical setting.