
Longitudinal Clival Fracture: A Lethal Injury Survived
Iman Feiz-Erfan, MD
Mauro A. T. Ferreira, MD
Eric M. Horn, MD, PhD
Harold L. Rekate, MD
Scott R. Petersen, MD*
Division of Neurological Surgery, Barrow Neurological Institute and *Del E. Webb Trauma Center, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
Clival fractures result from high-energy impacts and tend to be lethal or associated with significant neurological deficits. A rare patient who had a longitudinal clival fracture with an excellent outcome is presented.
Key Words: clivus, longitudinal clival fracture
Fractures involving the clivus are rare and typically fatal. Therefore, a significant number of clival fractures are detected postmortem. Computed tomography (CT) with bone window is the primary imaging modality to diagnose this condition, which is often missed on plain skull radiography.
Illustrative Case
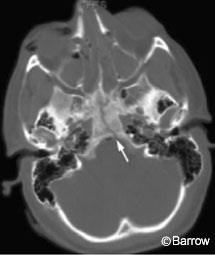
A 22-year-old male crashed into a wall while riding his motorcycle without a helmet. He sustained an acute subdural hematoma and was admitted as a Level 1 trauma. A longitudinal clival fracture (Fig. 1), frontal bone fractures, and frontal cerebral contusions were diagnosed on CT bone and soft tissue windows. He also had multiple fractures of his extremities and facial lacerations. After his cerebral condition was stabilized, he underwent primary repair of his frontal bone and facial fractures. He could follow commands with all extremities immediately after resuscitation but was left intubated. Cerebral angiography revealed no injury to his intracranial vasculature. Initially, cranial nerve (CN) deficits could not be elicited on examination, but he later developed bitemporal hemianopsia. He developed diabetes insipidus, which was successfully managed medically. A lumboperitoneal (LP) shunt treated his cerebrospinal fluid (CSF) leak successfully. He was discharged home 5 weeks after injury. His neurological level of functioning was otherwise intact, and his other injuries were healing appropriately. One month after discharge, his LP shunt occluded and was revised. He regained his baseline level of cerebral functioning with the exception of the bitemporal hemianopsia, which had improved 6 weeks after discharge.
Discussion
Clival fractures have been classified as longitudinal, transverse, and oblique. Longitudinal and transverse fractures represent about 75% of clival fractures. These two fracture types are associated with slightly different patterns of neurovascular injury. Longitudinal clival fractures most often are associated with injury to the vertebrobasilar system. Dissection, vessel occlusion, and subsequent ischemic damage to critical neural structures like the brainstem follow. Transverse fractures tend to involve the anterior circulation. All fracture types can be associated with CN deficits, especially involving CN III through VI. CSF leaks and the development of diabetes insipidus are also common.
Longitudinal fractures of the clivus are rarely associated with no permanent significant neurological damage. As demonstrated by this case, however, such fractures may well be compatible with a normal level of neural functioning if associated complications and systemic trauma are managed appropriately.
Acknowledgments
The authors thank Mr. Curtis T. Mundy and Mr. Andrew Durano for their help in preparing this manuscript.