
The Management of Cranial and Spinal CSF Leaks
G. Michael Lemole Jr., MD
Jeffrey S. Henn, MD
Joseph M. Zabramski, MD
Volker K. H. Sonntag, MD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
The term cerebrospinal fluid (CSF) leak refers to any disruption of the arachnoid and dura that allows CSF to escape to an extradural space. CSF leaks can occur anywhere along the craniospinal axis. The most common clinical manifestation of cranial CSF leaks is rhinorrhea or otorrhea. Leakage along spinal pathways can cause severe postural headaches such as those that complicate spinal puncture. Occasionally, recurrent bouts of bacterial meningitis are the only clue to diagnosis. Treatment options range from bedrest and drainage of CSF to direct surgical repair by a variety of approaches. Management depends on the suspected location, cause, and presenting symptoms of the CSF leak. The details of the senior authors’ approach to the evaluation and treatment of cranial and spinal CSF leaks are reviewed.
Key Words: cerebrospinal fluid (CSF), CSF fistula, CSF leak
The diagnosis and management of the patient with a cerebrospinal fluid (CSF) leak depend on the location of the leak, its etiology, and the patient’s presenting symptoms. When a leak is associated with external drainage of CSF via the paranasal sinuses, external ear, or a cutaneous tract, it is more appropriately referred to as a CSF fistula. In the literature, however, the distinction between these terms has become blurred, and CSF fistula and CSF leak are used interchangeably.
CSF leaks can result from diverse etiologies, including trauma, hydrocephalus, tumor, infection, and iatrogenic and idiopathic causes.[60] Clinical manifestations range from frank drainage of CSF that is easily recognized to slow, intermittent leakage that can be difficult to diagnose. Localization of a CSF leak can also prove challenging. The pertinent anatomy and mechanisms of formation of cranial and spinal CSF leaks must be understood to diagnose and treat these lesions properly. A clear understanding of their natural history is also mandatory for making sound management decisions.
This article examines the natural history, diagnosis, and treatment of CSF leaks involving the skull base and spinal column. The first section concentrates on cranial CSF fistulas; the second section addresses spinal CSF leaks, including their relationship to symptomatic intracranial hypotension.
Historical Background
In the second century A.D. Galen described the leakage of CSF after cranial trauma, but it was not considered a pathologic process until the mid17th century.[85] In 1826 Miller[54] noted nasal flow of spinal fluid in a child with hydrocephalus. In 1899 St. Clair Thomson[77] coined the term rhinorrhea in a report describing a group of patients with spontaneous nasal CSF leaks. In 1923 Grant[33] first proposed closing a traumatic dural defect. He reported a 19-year-old male with rhinorrhea and pneumocephalus following an automobile collision. He stated, “We felt that an attempt should be made to find and close the tear in the dura through which the air had entered.” Profuse bleeding from the dura foiled Grant’s proposed surgical intervention. In 1926 Dandy reported the first successful operative repair of a CSF leak.[23] He closed a traumatic dural tear over a frontal sinus fracture using muscle and fascia lata.
During the next several decades, a better understanding of the natural history of traumatic and spontaneous CSF fistulas was obtained. The earliest efforts to identify the site of a leak included instilling dyes into the CSF space. The dyes, however, were found to be neurotoxic and are no longer recommended.[5,60,85]
Other intrathecal markers for documenting CSF leakage were developed. In the 1950s, radioactive isotopes were first used and injected into the CSF space for diagnostic purposes.[21] Since then refinements in the radioactive tracers used for these procedures have improved the overall efficacy of the technique.
The development of computed tomography (CT) and the introduction of water-soluble contrast agents for intrathecal use, such as metrizamide, greatly improved the diagnosis and localization of CSF leaks. Diagnostic techniques are still evolving, and recent successes with magnetic resonance (MR) imaging suggest that it too may become a valuable tool.
Normal CSF Physiology
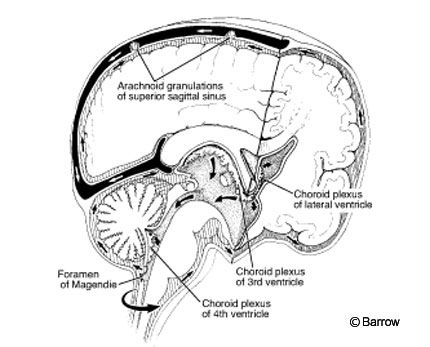
CSF is formed in the cerebral ventricles by the choroid plexus and through transependymal flow of parenchymal fluid. CSF communicates directly with the basal subarachnoid cisterns through the foramina of Magendie and Luschka in the posterior fossa. The subarachnoid space is defined by the potential volume between the pial lining over the neural parenchyma and the arachnoid layer of the meninges. Multiple trabeculae traverse the space between these two layers. The arachnoid layer does not directly follow the conformations of the underlying brain parenchyma and thus forms pockets or cisterns through which the CSF percolates. CSF exiting the fourth ventricle flows freely through the basal cisterns down around the spinal cord and up and over the cerebral convexities to be reabsorbed into the venous blood stream through arachnoid granulations in the superior sagittal sinus (Fig. 1).
CSF is thought to act as a physiological shock absorber that buffers the neuroparenchyma from direct trauma. It has also been proposed that CSF is analogous to lymph for the nervous system.[7] The process of the formation, flow, and reabsorption of CSF is dynamic. The entire volume of the CSF space is about 150 ml, and almost 500 ml of CSF are produced each day. Therefore, the volume of CSF is replaced about three times a day.
Classification of Cranial CSF Leaks
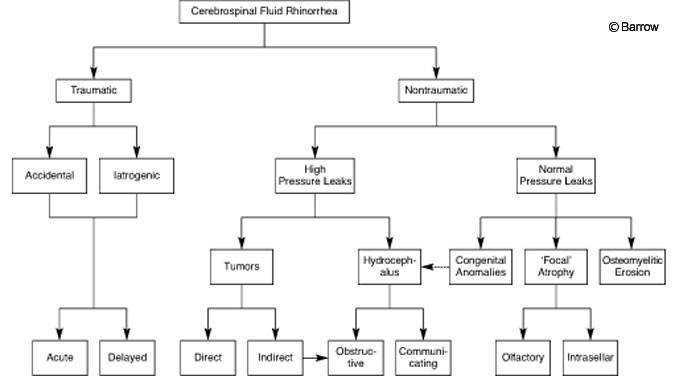
In 1937 Cairns[13] offered the first classification of CSF rhinorrhea, dividing CSF fistula into acute, delayed, traumatic, operative, and spontaneous groups. This scheme was further refined by differentiating between primary spontaneous or idiopathic rhinorrhea and secondary spontaneous rhinorrhea (i.e., rhinorrhea with an underlying etiology such as a tumor or hydrocephalus). Ommaya[60] classified all CSF leaks as traumatic or nontraumatic, dividing each based on whether the underlying CSF dynamics reflected high or low pressure. Traumatic etiologies included accidental trauma to the cranium or spinal axis as well as iatrogenic injuries. Nontraumatic CSF leaks included those caused directly or indirectly by tumors, those caused by hydrocephalus, those initiated by infection, and those thought to arise from congenital anomalies or focal atrophy (Fig. 2). Groups within Ommaya’s classification scheme overlap (e.g., when occult traumatic fractures of the skull manifest with delayed CSF leaks), but the system is useful when the natural history of each group is considered.
Traumatic Cranial CSF Leaks
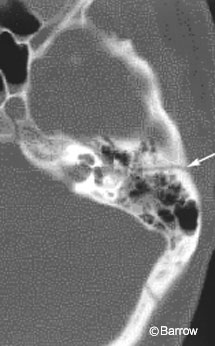
Trauma is the most common origin of cranial CSF leaks,[5,60] responsible for as many as 90% of the cases of CSF rhinorrhea.[85] Fractures through the floor of the anterior cranial fossa may extend directly into the paranasal sinuses. If the dura and arachnoid are also torn by the trauma, a CSF fistula may result, presenting with rhinorrhea. Fractures through the petrous bone can cause CSF leaks because of the proximity of the middle ear, particularly longitudinal fractures (Fig. 3) that run through the middle ear.[5] Eighty percent of traumatic CSF leaks involve nasal pathways while 20% involve aural pathways.[1] Penetrating head injuries can also produce CSF leaks at any location.
Posttraumatic CSF leaks occur in 2 to 3% of patients with head injury. The rate is highest in patients with anterior skull base fractures. Brodie and Thompson[11] reported a 14.5% incidence of CSF leaks in a review of 820 cases of temporal bone fractures. In patients with facial fractures, the incidence of CSF rhinorrhea is as high as 25%.[26] The demographics of this population of patients parallel those of the trauma statistics, with the majority of cases involving young adult males, 18 to 25 years of age. Posttraumatic CSF leaks are uncommon in young children and rare in those younger than 2 years of age.[5,15,44] The apparent immunity of infants to traumatic CSF leaks likely results from the flexibility of the skull base, especially the cartilaginous nature of the ethmoids, and the poor development of the frontal and sphenoid air sinuses. Beyond the age of 5 years, the frontal air sinuses progressively enlarge reaching adult dimensions by 14 years of age. Interestingly, there is little correlation between the severity of head injury and the occurrence of a CSF leak. Mincy[55] reported that almost 50% of patients with posttraumatic CSF leaks suffered a brief or no loss of consciousness and had no neurological deficits.
Posttraumatic CSF leaks are divided into two categories: (1) those in which the leak is apparent immediately or soon after trauma and (2) those in which the leak commences weeks to months after head injury. In 60% of patients, the CSF leak is apparent with the first few days of injury and is diagnosed in 95% of patients within 3 months.[85] The delayed onset of CSF rhinorrhea or otorrhea after head trauma may reflect the resolution of a hematoma, cerebral edema, or both in the region of the fracture. CSF leaks can also complicate the delayed reduction of nasal or facial fractures. In a small number of patients the onset of posttraumatic CSF leakage may be delayed for years, with the longest reported delay being 36 years.[68]
Symptoms of cranial CSF leak include frank rhinorrhea or otorrhea. CSF leakage can also be intermittent or apparent only with a change in posture. Anosmia is a common complaint, particularly when the cribriform plate is involved.[60] Meningitis is the most significant risk associated with traumatic CSF leaks and has been reported to complicate 25 to 50% of untreated cases.[1,11,60] The risk of meningitis increases with the duration of CSF leakage. In a review of 122 cases of posttraumatic CSF leaks, meningitis was reported in only 3% of patients when the leak was treated successfully within one week compared to 23% for those with leaks lasting longer than one week.[11] Pneumococcal infection is the most common cause of meningitis in this population.
Unlike adult patients with meningitis from other causes, the course of posttraumatic meningitis is relatively benign. Prompt treatment with appropriate antibiotics can minimize morbidity and mortality rates and permits a rational approach to the treatment of the CSF fistula without the need for “emergency” surgery.
Under the scheme proposed by Ommaya, CSF leaks resulting from surgical procedures are classified as traumatic (Fig. 2). Complications of CSF leak are more frequent in those procedures that involve the ethmoid sinuses and mastoid air cells. The rates of CSF leaks associated with acoustic neuromas are 5 to 10%,[39,83] and those associated with transsphenoidal surgery are 3 to 6%.[19,80] In the patient with a pneumatized anterior clinoid, drilling to expose the proximal internal carotid artery can lead to a postoperative CSF leak. Careful waxing of exposed air cells, combined with the use of fibrin glue and multiple-layer closures, can help minimize these risks.
Nontraumatic or Spontaneous Cranial CSF Leaks
Ommaya[60] divided spontaneous CSF leaks into normal- and high-pressure categories (Fig. 2). High-pressure leaks related to longstanding increases in intracranial pressure (ICP) account for about 45% of spontaneous CSF leaks.[85] Specific etiologies include congenital and acquired hydrocephalus as well as other abnormalities associated with increased ICP, including Crouzon’s disease, Albers-Schönberg disease, and mass effect from slow-growing tumors. High-pressure CSF leaks are not a result of direct invasion of the skull base. The remaining 50 to 60% of spontaneous CSF leaks occur in the presence of normal ICP.[84,85]
Nontraumatic causes of normal pressure CSF leaks include intracranial tumors that directly invade the skull base, infections such as osteomyelitis and tuberculosis, meningoceles and meningoencephaloceles, and defective development or atrophy of the olfactory bulbs that exposes the thin perforated bone of the lamina cribrosa to pulsations of CSF. Even in the presence of normal ICP, it is postulated that the constant pulsation of CSF can cause the gradual dilation of these pouches with their eventual rupture and leakage of CSF. Increased ICP from any cause would be expected to accelerate this process. Kaufman et al.[48] have emphasized the importance of pneumatization of the middle cranial fossa floor in the etiology of spontaneous CSF leaks. The authors hypothesize that pneumatization of the middle fossa floor in combination with the normal pulsations of CSF thin the dura and bone and result in small pits and holes. Continuation of this process could lead to bony and dural dehiscence, with herniation and rupture of arachnoid diverticula.
Nontraumatic or spontaneous CSF leaks are much less common than their traumatic counterparts. Females are affected more frequently than males (2:1), and presentation is most common in the fourth to fifth decades.[60] Rhinorrhea, induced by coughing or sneezing, is the most frequent symptom. Patients also may complain of a salty or metallic taste in the back of their throat. Intermittent symptoms can persist for years, misdiagnosed as allergic rhinitis or postnasal drip.[60] The occurrence of meningitis is rare but may be the only clue to diagnosis. In contrast to traumatic CSF leaks, anosmia is rare.
Diagnosis and Localization of Cranial CSF Leaks
The management of patients with a CSF fistula requires confirmation of the diagnosis and localization of the responsible defect. Sometimes the presence of a CSF leak is obvious, as in the case of acute trauma associated with pneumocephalus, but it can also be extremely challenging to diagnose. A subtle CSF leak may often be demonstrated by having the patient sit up, lean forward, and flex the neck after lying supine overnight. If CSF has collected in the sphenoid sinus overnight, flexion of the head in an upright position will discharge the fluid through the sphenoid ostia, which are situated halfway up the anterior wall of the sphenoid sinus. This momentary profuse discharge (called a positive “reservoir sign”) may help establish the diagnosis as well as allow ample fluid to be collected for chemical analysis.
If sufficient blood-free drainage can be collected, measurement of the patient’s glucose level of the fluid can be used to confirm the diagnosis of a CSF leak. The glucose level in CSF is normally greater than 30 mg/100ml.[30,42] After trauma, the results of glucose analysis are unreliable because drainage will be contaminated with blood.[5] Under such circumstances, the presence of the specific CSF marker, b2-tranferrin, is diagnostic for a CSF fistula.[63] Assays for this marker usually must be sent to specialized laboratories, and thus one or two days may be required before results are available. A crude but relatively reliable test involves observing the pattern created by the suspected drainage on clean linen. Bloody CSF characteristically produces a ring or “halo” pattern with the blood carried to the periphery of the fluid stain.
All patients with head injury and basal skull fractures should undergo evaluation for a possible CSF leak. As noted above, patients with specific fracture patterns that involve the frontal or ethmoidal sinuses and those that extend parallel to the long axis of the petrous bone are at highest risk for developing a CSF fistula. CT imaging with bone window settings is the procedure of choice for the evaluation of skull base fractures. Coronal CT imaging can be helpful in patients with facial fractures that extend into the skull base. Intracranial air is easily recognized on CT, and in the absence of an apparent leak provides evidence for the presence of a CSF fistula.
In patients with spontaneous CSF leaks, the diagnosis may be more difficult to confirm because the leak may be small and intermittent drainage is common. In such cases, radionuclide cisternography combined with the use of nasal pledgets and maneuvers to increase ICP (e.g., head positioning and straining) may allow the CSF leak to be diagnosed.[52,85] Cotton pledgets are placed adjacent to the major ostia of the paranasal sinuses. The labeled pledgets are removed after 12 to 24 hours, and the level of radioactivity is counted. Elevated counts confirm the presence of a CSF leak and may even help identify its location.
Accurate localization of the site of the CSF fistula is essential whenever surgical intervention is being considered. High-resolution CT imaging will identify the bony defect and the site of the CSF fistula in a large percentage of cases. If there is any question regarding the site of the fistula, CT imaging can be combined with metrizamide cisternography. The metrizamide contrast is injected either via the lumbar subarachnoid space or a lateral C1-C2 puncture. The contrast is injected under fluoroscopic guidance, and the patient is positioned head down to bring the contrast into the basal cisterns. When possible, the patient is placed prone in the CT scanner with the neck gently hyperextended to encourage gravity drainage of CSF through the fistula. Fine 3 mm x 3 mm coronal CT sections are obtained. Additional sections in the coronal and axial planes may be necessary to visualize the fistula. In patients with low-flow fistulas, delayed imaging may be useful.[74] Recent reports have advocated MR imaging as a noninvasive method for localizing the site of a CSF fistula. Several groups have suggested that its sensitivity rivals that of CT cisternography;[24,27,58] however, this view is not yet widely accepted.
When the diagnosis of a CSF fistula has been confirmed but its location remains elusive, endoscopic techniques may be helpful. Endoscopy combined with intrathecal or topically applied fluorescein permits visualization of the site of the CSF leak.[14,41,45] In extreme cases an open surgical exploration without prior localization may be required to identify the site of CSF leakage. Direct repair of the fistula is usually attempted at the time of the endoscopic or surgical exploration.
Treatment of Cranial CSF Leaks
The treatment of CSF fistulas can be divided into nonoperative and operative management. The choice of treatment depends on the etiology and severity of the CSF leak as well as on the timing and mode of presentation. The general rule of thumb is to begin with the least invasive treatment and escalate as necessary. This approach is particularly useful for traumatic CSF leaks.
The initial management of patients with a traumatic CSF leak typically includes bed rest and elevation of the head. Patients are encouraged to avoid coughing, sneezing, nose blowing, and any straining that would increase ICP. Stool softeners and laxatives are given as necessary to avoid straining during bowel movements. Using this simple approach, 70 to 85% of cases of traumatic CSF rhinorrhea will resolve within 7 days, and almost all cases of traumatic otorrhea will resolve.[11,55,60]
Traumatic CSF leaks that do not respond to conservative measures within 5 to 7 days should be considered for more invasive treatment.[1,60,73] Intermittent lumbar taps and placement of a lumbar drain are effective methods of reducing ICP and of encouraging closure of the CSF fistula. All patients with lumbar drains should be monitored in an intensive care unit. Rapid or excessive drainage of CSF is dangerous and must be avoided. We prefer to begin drainage at 5 to 10 cc an hour. The height of the drain is titrated to maintain a slow, steady flow rate. The drain is closed once the desired volume for any given hour has been obtained. The drain also can be closed to allow the patient to sit up at bedside for meals. Overdrainage of CSF is associated with headache, nausea, and vomiting and can progress rapidly to coma with signs of tentorial herniation. If the patient’s condition deteriorates, the drain should be closed immediately and the patient placed in a flat or slight Trendelenburg (head down) position. Oxygen (100%) is administered, and a CT scan is obtained to assess for the presence of intracranial air and to define the cause of the deterioration more precisely. The presence of pneumocephalus is a contraindication to continued lumbar CSF drainage.
The use of prophylactic antibiotics in patients with traumatic CSF fistulas remains controversial. In 1997 Brodie[10] published a meta-analysis suggesting that prophylactic antibiotics might be beneficial; however, numerous other studies, including a second meta-analysis in 1998 by Villalobos et al.,[81] have failed to demonstrate that they lower infection rates. The emergence of drug-resistant bacteria and reports of infection with more virulent organisms have heightened concerns about the indiscriminate use of antibiotics.[17,25] In one intensive care unit, the widespread use of prophylactic antibiotics led to an epidemic of Klebsiella meningitis that resulted in eight deaths.[62] Based on the available literature, the prophylactic use of antibiotics in patients with CSF leaks appears to be ineffective and cannot be recommended. This caveat does not include the short-term perioperative use of antibiotics beginning immediately before surgery for the repair of CSF fistula.
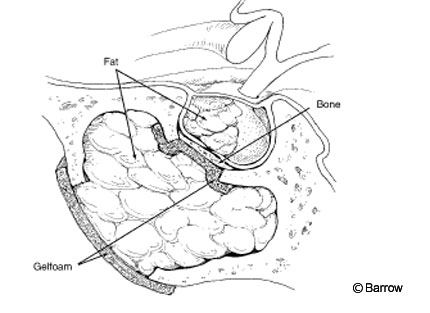
Operative management is reserved for traumatic CSF leaks that fail to respond to conservative measures. Surgical procedures can be divided into intracranial and extracranial approaches. Extracranial approaches are limited to the anterior cranial fossa and paranasal sinuses. Endoscopic techniques have broadened the indications and improved the results associated with the extracranial repair of CSF leaks.[57,66,78] Success rates as high as 90% have been reported.[16] Under direct endoscopic visualization, a leak often can be identified and the sinus into which it drains can be obliterated by packing it with fat or muscle (Fig. 4).
Other techniques described in conjunction with extracranial techniques include mobilization of mucocutaneous flaps and combinations of autologous tissues with fibrin glue.[2,20,59,79] A theoretical disadvantage of extracranial approaches is that the patch is less secure than when it is placed intradurally. With intradural repair the patch is held firmly against the defect by the brain and normal CSF pressure. Wormald and McDonogh[82] recently addressed this concern: They described the endoscopic repair of CSF leaks using a “bath-plug” technique to seal the defect from the intradural side.
Typically, intracranial procedures are reserved for patients with defects that are not amenable to extracranial endoscopic techniques, including patients with extensive skull base fractures, comminuted fractures with displaced fragments that require reduction, and fractures associated with intracranial hemorrhages or contusions that ordinarily would require craniotomy for treatment.
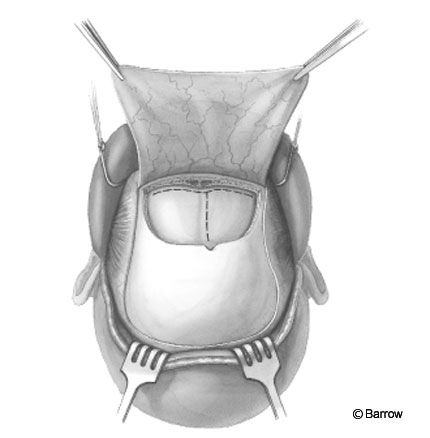
A bicoronal incision is usually employed (Fig. 5), and the craniotomy is tailored to the extent of the bony defects and associated intracranial pathology. When bony defects are lateralized to one side, a frontal or pterional craniotomy may be used. The patient’s head is positioned to permit gravity to aid in retraction of the frontal lobes. Lumbar drainage of CSF and the intraoperative use of mannitol can further minimize the need for retraction. Depending on the location of the skull base defect, the operative microscope is an invaluable adjunct. Dural defects can be repaired directly by suturing, but autologous tissue grafts are frequently employed.
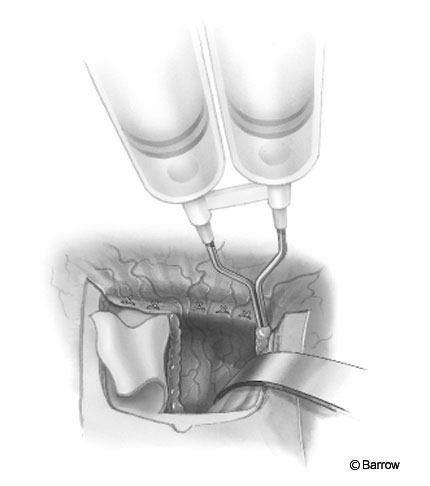
The authors prefer a vascularized periosteal graft, but fascia lata or various commercially available dural substitutes can be used. Grafts can be sutured in place, but most surgeons use fibrin glue to reinforce the closure (Fig. 6). In clinical and laboratory studies, fibrin glue has been shown to significantly enhance dural closure and to reduce the risk of CSF leakage.[35,59,67]
Operative management of CSF leaks may require repair of bony defects. Small defects can be filled with bone dust and fibrin glue. For larger defects, split thickness bone autografts, held in place with fibrin glue or one of the available microplate systems, are ideal. Facial fractures should be reduced prior to or in combination with procedures for closure of a traumatic CSF fistula.[22,26,75] The early treatment of facial fractures may enhance the spontaneous resolution of traumatic CSF leaks while delayed reduction may lead to a recurrence.
The same principles apply to closing CSF fistulas that arise in the middle or posterior fossa. In the middle fossa, leakage can occur through air cells in the lesser sphenoid wing or floor of the temporal fossa. In the latter cases, an extradural approach may be used to close the defect.[37,65] Ultimately, combined intra- and extradural approaches may be necessary.[4] In rare cases a mastoidectomy may be needed to obliterate the offending air cells.[34,36] The correct surgical approach is the one that will permanently stop the CSF leak with the least risk to the patient.
Postoperative CSF leaks are often responsive to conservative measures.
CSF leakage after transphenoidal surgery initially should be treated with best rest and lumbar drainage of CSF. If the leak persists despite lumbar drainage, repacking of the sphenoid sinus is indicated.
CSF leaks complicate 10 to 20% of the resections of cerebellopontine angle tumors, particularly if the approach involves extensive drilling of the petrous-temporal bone.[9,28,31,50,72] The risk of a CSF leak can be minimized by scrupulously packing opened air cells with wax or fat as well as by filling any bony defect with fatty tissue. Bed rest and lumbar drainage are usually sufficient to stop these leaks. Subgaleal collections may respond well to aspiration and a simple compression dressing. A percutaneous technique for aspirating fluid and injecting fibrin glue to close a subgaleal fistula has also been described.[53] Recurrent subgaleal collections should raise suspicion of hydrocephalus.
In contrast to traumatic CSF leaks, spontaneous CSF leaks are unlikely to respond to nonoperative intervention. Treatment is directed at identifying the site of the fistula and treating the underlying cause (i.e., resection of a mass lesion causing increased ICP or insertion of a shunt for hydrocephalus). The presence of hydrocephalus may be difficult to assess in patients with an active CSF leak. Careful follow-up with serial CT imaging studies may demonstrate evidence of previously unsuspected hydrocephalus. Delayed failure of an apparently successful repair should raise the clinical suspicion of hydrocephalus. In such cases, radiolabeled cisternography may show altered CSF dynamics such as the reflux of isotope into the ventricles.
Spinal CSF Leaks
Like their cranial counterparts, CSF leaks involving the spinal axis can be divided into traumatic and nontraumatic (or spontaneous) categories. Traumatic spinal CSF leaks include iatrogenic lesions resulting from surgical, therapeutic, or diagnostic procedures. Diagnosis is often straightforward as in the case of the patient with a penetrating trauma and cutaneous CSF leak or the patient with a spinal headache following lumbar puncture. Traumatic CSF fistulas from the spinal subarachnoid space to the pleural space have been described.[3,32,69] Symptoms of intracranial hypotension (severe postural headache) and the presence of pleural fluid collections should suggest the diagnosis. The presence of b2-tranferrin in pleural fluid is diagnostic of a CSF leak.
Spontaneous spinal CSF leaks can be difficult to diagnose, but the similarity of the symptoms to those of spinal headache after lumbar puncture should suggest the diagnosis. Severe headaches, nausea, and vomiting often lead to MR imaging of the brain. Contrast-enhanced MR images demonstrate diffuse, intense dural enhancement that can be mistaken for meningitis or for metastatic or inflammatory disease.[8,12,18] Subdural fluid collections consistent with hygromas are reported in 60 to 70% of patients.[70] Caudal displacement of cerebellar tonsils and obliteration of the basal cisterns are usually present.[8,12,18,70]
Other clinical features may be more alarming: cranial neuropathies, typically uni- or bilateral abducens palsy, transient visual disturbances, photophobia, auditory disturbances, facial numbness or weakness, and stupor from traction and downward displacement of the brain stem.[6,38,49,71] The literature regarding spontaneous spinal CSF leaks is somewhat confusing. Despite recognition that these symptoms are the result of spontaneous spinal CSF leaks, patients are grouped under the diagnosis of “spontaneous intracranial hypotension.”

Radionucleotide cisternography is fairly characteristic in patients with spontaneous spinal CSF leaks. In patients with an active leak, escape of the CSF from the spinal subarachnoid space leads to rapid uptake of the tracer in the blood stream, demonstrated by the early appearance of the tracer in the kidneys and bladder.[46,56,64,70] Occasionally, the site of a spinal CSF leak is identified, but often the leak is below the resolution of the study.[46,70]
CT myelography is required to localize the leak if surgery is considered and may reveal the underlying anatomic deficit causing the leak, such as a meningeal diverticulum.[29,70] Myelography (Fig. 7) is often useful for localizing the general vicinity of the leak for subsequent CT scanning.
If myelography fails to localize the area of the leak, CT imaging should be obtained along the entire spinal axis. MR imaging studies of the spine may show extraaxial CSF collections that help localize the site of the leak, but experience with spinal MR imaging in patients with spontaneous spinal CSF leaks is limited.[51]
Treatment of Spinal CSF Leaks
Treatment of spinal CSF fistulas follows the paradigm described for cranial CSF leaks. In the case of traumatic and postoperative CSF leaks, bed rest and a short course of diversionary lumbar drainage are often adequate. Postoperative leaks often respond to simple oversewing of the wound, but patients should be followed closely for signs that suggest continued leakage such as postural headaches or the development of a pseudomeningocele. When the fistula fails to respond to conservative measures, operative exploration should be considered.
In postoperative cases careful inspection often reveals a previously unnoticed dural tear that can be repaired with direct suture technique, application of fibrin glue, or both. With spinal fluid leaks related to penetrating trauma, the approach is dictated by the site of the fistula, which is best defined by CT myelography. Percutaneous techniques for delivering fibrin glue to the site of the leak have had some success.[40,61]
The management of spontaneous spinal CSF leaks begins with fluid replacement and bed rest to relieve the symptoms of intracranial hypotension. Medical treatment options include intravenous caffeine infusions, glucocorticoids, and various nonsteroidal anti-inflammatory agents, mineralocorticoids, and salt infusions. A more direct and, in our experience, more efficacious treatment is a lumbar epidural blood patch. The success of this procedure may be explained by the findings of Szeinfeld et al.[76] that blood injected into the lumbar epidural spaces spreads rostrally and caudally to involve eight or more spinal segments. Fortunately, 60 to 70% of patients will respond to these conservative measures.[8,43,70] Surgical intervention should be considered only if symptoms recur after treatment with two adequate blood patches.
Most documented leaks are located at the cervicothoracic junction or in the thoracic spine.[77] Where surgical confirmation has been available, the leaks have been the result of ruptured meningeal diverticula. Surgical ligation of leaking meningeal diverticula has been associated with good outcomes.[43,71] Recently, epidural patching with fibrin glue has been used to successfully treat patients with spontaneous spinal CSF leaks who were unresponsive to epidural blood patches.[47]
The etiology of most meningeal diverticula is unknown, and it is unclear whether these lesions are congenital or acquired. It is likely, however, at least in some cases, that an underlying weakness of the spinal meninges is involved, predisposing the patient to develop meningeal diverticula.
Conclusion
CSF leaks can occur anywhere along the craniospinal axis. Trauma is the most frequent cause of cranial CSF leaks, but spontaneous cases are being recognized increasingly, particularly along the spinal axis where they manifest clinically as spontaneous intracranial hypotension. The selection of treatment depends on the etiology and severity of the CSF leak; however, the general rule is to start with conservative measures and to escalate to more invasive procedures as necessary. Exceptions requiring direct operative intervention might include patients with large amounts of intracranial air, extensive skull base fractures, or chronic CSF leakage.
References
- Aarabi B, Leibrock LG: Neurosurgical approaches to cerebrospinal fluid rhinorrhea. Ear Nose Throat J 71:300-305, 1992
- Anand VK, Murali RK, Glasgold MJ: Surgical decisions in the management of cerebrospinal fluid rhinorrhoea. Rhinology 33:212-218, 1995
- Assietti R, Kibble MB, Bakay RA: Iatrogenic cerebrospinal fluid fistula to the pleural cavity: Ca
- Beckhardt RN, Setzen M, Carras R: Primary spontaneous cerebrospinal fluid rhinorrhea. Otolaryngol Head Neck Surg 104:425-432, 1991
- Bergman TA, Rockswold GL: Cerebrospinal fluid fistulae, in Youmans JR (ed): Youmans Neurological Surgery. A Comprehensive Guide to the Diagnosis and Management of Neurosurgical Problems. Philadelphia: W.B. Saunders, 1996, pp 1840-1852
- Berlit P, Berg-Dammer E, Kuehne D: Abducens nerve palsy in spontaneous intracranial hypotension. Neurology 44:1552, 1994
- Binhammer RT: CSF anatomy with emphasis on relations to nasal cavity and labyrinthine fluids. Ear Nose Throat J 71:292-299, 1992
- Blank SC, Shakir RA, Bindoff LA, et al: Spontaneous intracranial hypotension: Clinical and magnetic resonance imaging characteristics. Clin Neurol Neurosurg 99:199-204, 1997
- Brennan JW, Rowed DW, Nedzelski JM, et al: Cerebrospinal fluid leak after acoustic neuroma surgery: Influence of tumor size and surgical approach on incidence and response to treatment. J Neurosurg 94:217-223, 2001
- Brodie HA: Prophylactic antibiotics for posttraumatic cerebrospinal fluid fistulae. A meta-analysis. Arch Otolaryngol Head Neck Surg 123:749-752, 1997
- Brodie HA, Thompson TC: Management of complications from 820 temporal bone fractures. Am J Otol 18:188-197, 1997
- Bruera OC, Bonamico L, Giglio JA, et al: Intracranial hypotension: The nonspecific nature of MRI findings. Headache 40:848-852, 2000
- Cairns H: Injuries of the frontal and ethmoidal sinuses with special reference to cerebrospinal fluid rhinorrhoea and aeroceles. J Laryngol Otol 52:589-623, 1937
- Calcaterra TC: Extracranial surgical repair of cerebrospinal rhinorrhea. Ann Otol Rhinol Laryngol 89:108-116, 1980
- Caldicott WJ, North JB, Simpson DA: Traumatic cerebrospinal fluid fistulas in children. J Neurosurg 38:1-9, 1973
- Casiano RR, Jassir D: Endoscopic cerebrospinal fluid rhinorrhea repair: Is a lumbar drain necessary? Otolaryngol Head Neck Surg 121:745-750, 1999
- Choi D, Spann R: Traumatic cerebrospinal fluid leakage: Risk factors and the use of prophylactic antibiotics. Br J Neurosurg 10:571-575, 1996
- Christoforidis GA, Mehta BA, Landi JL, et al: Spontaneous intracranial hypotension: Report of four cases and review of the literature. Neuroradiology 40:636-643, 1998
- Ciric IS, Tarkington J: Transsphenoidal microsurgery. Surg Neurol 2:207-212, 1974
- Citardi MJ, Cox AJ3, Bucholz RD: Acellular dermal allograft for sellar reconstruction after transsphenoidal hypophysectomy. Am J Rhinol 14:69-73, 2000
- Crow HJ, Keogh C, Northfield DWC: The localisation of cerebrospinal-fluid fistulae. Lancet 2:325-327, 1956
- Daly DT, Lydiatt WM, Ogren FP, et al: Extracranial approaches to the repair of cerebrospinal fluid rhinorrhea. Ear Nose Throat J 71:311-313, 1992
- Dandy WE: Pneumocephalus (intracranial pneumatocele or aerocele). Arch Surg 12:949-982, 1926
- El Gammal T, Sobol W, Wadlington VR, et al: Cerebrospinal fluid fistula: Detection with MR cisternography. AJNR Am J Neuroradiol 19:627-631, 1998
- Eljamel MS: Antibiotic prophylaxis in unrepaired CSF fistulae. Br J Neurosurg 7:501-505, 1993
- Eljamel MS: Fractures of the middle third of the face and cerebrospinal fluid rhinorrhoea. Br J Neurosurg 8:289-293, 1994
- Eljamel MS, Pidgeon CN: Localization of inactive cerebrospinal fluid fistulas. J Neurosurg 83:795-798, 1995
- Fishman AJ, Hoffman RA, Roland JT, Jr., et al: Cerebrospinal fluid drainage in the management of CSF leak following acoustic neuroma surgery. Laryngoscope 106:1002-1004, 1996
- Fitzgerald LF, Sandlin M, Carrier D, et al: Spontaneous intracranial hypotension: Myelographic findings. Case illustration. J Neurosurg 92:188, 2000
- Gadeholt H: The reaction of glucose-oxidase test paper in normal nasal secretion. Acta Otolaryngol (Stockh) 58:271-272, 1964
- Gillman GS, Parnes LS: Acoustic neuroma management: A six-year rieview. J Otolaryngol 24:191-197, 1995
- Godley CD, McCabe CJ, Warren RL, et al: Traumatic subarachnoid-pleural fistula: Case report. J Trauma 38:808-811, 1995
- Grant FC: Intracranial aerocele following fracture of the skull: Report of a case with review of the literature. Surg Gynecol Obstet 36:251-255, 1923
- Grant IL, Welling DB, Oehler MC, et al: Transcochlear repair of persistent cerebrospinal fluid leaks. Laryngoscope 109:1392-1396, 1999
- Hadley MN, Martin NA, Spetzler RF, et al: Comparative transoral dural closure techniques: A canine model. Neurosurgery 22:392-397, 1988
- Hamilton JW, Foy PM, Lesser TH: Subtotal petrosectomy in the treatment of cerebrospinal fluid fistulae of the lateral skull base. Br J Neurosurg 11:496-500, 1997
- Harner SG, Laws ER, Jr.: Translabyrinthine repair for cerebrospinal fluid otorhinorrhea. J Neurosurg 57:258-261, 1982
- Horton JC, Fishman RA: Neurovisual findings in the syndrome of spontaneous intracranial hypotension from dural cerebrospinal fluid leak. Ophthalmology 101:244-251, 1994
- House WF, Hitselberger WE: Surgical complications of acoustic tumor surgery. Arch Otolaryngol 88:659-667, 1968
- Huch K, Kunz U, Kluger P, et al: Epidural blood patch under fluoroscopic control: Non-surgical treatment of lumbar cerebrospinal fluid fistula following implantation of an intrathecal pump system. Spinal Cord 37:648-652, 1999
- Hughes RG, Jones NS, Robertson JJ: The endoscopic treatment of cerebrospinal fluid rhinorrhoea: The Nottingham experience. J Laryngol Otol 111:125-128, 1997
- Hull HF, Morrow G: Glucorrhea revisited. Prolonged promulgation of another plastic pearl. JAMA 234:1052-1053, 1975
- Inenaga C, Tanaka T, Sakai N, et al: Diagnostic and surgical strategies for intractable spontaneous intracranial hypotension. Case report. J Neurosurg 94:642-645, 2001
- Jones DT, McGill TJ, Healy GB: Cerebrospinal fistulas in children. Laryngoscope 102:443-446, 1992
- Jones ME, Reino T, Gnoy A, et al: Identification of intranasal cerebrospinal fluid leaks by topical application with fluorescein dye. Am J Rhinol 14:93-96, 2000
- Kadrie H, Driedger AA, McInnis W: Persistent dural cerebrospinal fluid leak shown by retrograde radionuclide myelography: Case report. J Nucl Med 17:797-799, 1976
- Kamada M, Fujita Y, Ishii R, et al: Spontaneous intracranial hypotension successfully treated by epidural patching with fibrin glue. Headache 40:844-847, 2000
- Kaufman B, Nulsen FE, Weiss MH, et al: Acquired spontaneous, nontraumatic normal-pressure cerebrospinal fluid fistulas originating from the middle fossa. Radiology 122:379-387, 1977
- Kosmorsky GS: Spontaneous intracranial hypotension: A review. J Neuro-Ophthalmol 15:79-83, 1995
- Magliulo G, Sepe C, Varacalli S, et al: Cerebrospinal fluid leak management following cerebellopontine angle surgery. J Otolaryngol 27:258-262, 1998
- Matsumura A, Anno I, Kimura H, et al: Diagnosis of spontaneous intracranial hypotension by using magnetic resonance myelography. Case report. J Neurosurg 92:873-876, 2000
- McKusick KA, Malmud LS, Kordela PA, et al: Radionuclide cisternography: Normal values for nasal secretion of intrathecally injected 111In-DTPA. J Nucl Med 14:933-934, 1973
- Menovsky T, de Vries J, Bloss HG: Treatment of postoperative subgaleal cerebrospinal fluid fistulas by using fibrin sealant. Technical note. J Neurosurg 90:1143-1145, 1999
- Miller C: A case of hydrocephalus chronicus, with some unusual symptoms and appearance on dissection. Trans Med Chir Soc 2:243-248, 1826
- Mincy JE: Posttraumatic cerebrospinal fluid fistula of the frontal fossa. J Trauma 6:618-622, 1966
- Molins A, Alvarez J, Sumalla J, et al: Cisternographic pattern of spontaneous liquoral hypotension. Cephalalgia 10:59-65, 1990
- Nachtigal D, Frenkiel S, Yoskovitch A, et al: Endoscopic repair of cerebrospinal fluid rhinorrhea: Is it the treatment of choice? J Otolaryngol 28:129-133, 1999
- Nakayama Y, Tanaka A, Ueno Y, et al: Spontaneous cerebrospinal fluid leakage detected by magnetic resonance cisternography—case report. Neurol Med Chir (Tokyo) 39:251-254, 1999
- Nishihira S, McCaffrey TV: The use of fibrin glue for the repair of experimental CSF rhinorrhea. Laryngoscope 98:625-627, 1988
- Ommaya AK: Cerebrospinal fluid fistula and pneumocephalus, in Wilkins RH, Rengachary SS (eds): Neurosurgery. New York: McGraw-Hill, 1996, pp 2773-2782
- Patel MR, Louie W, Rachlin J: Postoperative cerebrospinal fluid leaks of the lumbosacral spine: Management with percutaneous fibrin glue. AJNR Am J Neuroradiol 17:495-500, 1996
- Price DJ, Sleigh JD: Control of infection due to Klebsiella aerogenes in a neurosurgical unit by withdrawal of all antibiotics. Lancet 2:1213-1215, 1970
- Reisinger PW, Hochstrasser K: The diagnosis of CSF fistulae on the basis of detection of beta 2-transferrin by polyacrylamide gel electrophoresis and immunoblotting. J Clin Chem Clin Biochem 27:169-172, 1989
- Renowden SA, Gregory R, Hyman N, et al: Spontaneous intracranial hypotension. J Neurol Neurosurg Psychiatry 59:511-515, 1995
- Robson AK, Clarke PM, Dilkes M, et al: Transmastoid extracranial repair of CSF leaks following acoustic neuroma resection. J Laryngol Otol 103:842-844, 1989
- Ross IB, Colohan AR, Black MJ: Extracranial repair of cerebrospinal fluid rhinorrhea. Can J Neurol Sci 17:320-323, 1990
- Rossitch E, Jr., Wilkins RH: Use of fibrin glue in neurosurgery, in Wilkins RH, Rengachary SS (eds): Neurosurgery. New York: McGraw-Hill, 1996, pp 623-624
- Salca HC, Danaila L: Onset of uncomplicated cerebrospinal fluid fistula 27 years after head injury: Case report. Surg Neurol 47:132-133, 1997
- Sarwal V, Suri RK, Sharma OP, et al: Traumatic subarachnoid-pleural fistula. Ann Thorac Surg 62:1622-1626, 1996
- Schievink WI, Meyer FB, Atkinson JL, et al: Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. J Neurosurg 84:598-605, 1996
- Schievink WI, Morreale VM, Atkinson JL, et al: Surgical treatment of spontaneous spinal cerebrospinal fluid leaks. J Neurosurg 88:243-246, 1998
- Sluyter S, Graamans K, Tulleken CA, et al: Analysis of the results obtained in 120 patients with large acoustic neuromas surgically treated via the translabyrinthine-transtentorial approach. J Neurosurg 94:61-66, 2001
- Spetzler RF, Wilson CB: Management of recurrent CSF rhinorrhea of the middle and posterior fossa. J Neurosurg 49:393-397, 1978
- Stone JA, Castillo M, Neelon B, et al: Evaluation of CSF leaks: High-resolution CT compared with contrast-enhanced CT and radionuclide cisternography. AJNR Am J Neuroradiol 20:706-712, 1999
- Stranc MF, Harrison DH: Primary treatment of craniofacial injuries. Rev Stomatol Chir Maxillofac 79:363-371, 1978
- Szeinfeld M, Ihmeidan IH, Moser MM, et al: Epidural blood patch: Evaluation of the volume and spread of blood injected into the epidural space. Anesthesiology 64:820-822, 1986
- Thomson St C: The Cerebrospinal Fluid: Its Spontaneous Escape from the Nose. London: Cassell, 1899
- Tolley NS: A clinical study of spontaneous CSF rhinorrhoea. Rhinology 29:223-230, 1991
- Van Den Abbeele T, Elmaleh M, Herman P, et al: Transnasal endoscopic repair of congenital defects of the skull base in children. Arch Otolaryngol Head Neck Surg 125:580-584, 1999
- VanGilder JC, Goldenberg IS: Hypophysectomy in metastatic breast cancer. Arch Surg 110:293-295, 1975
- Villalobos T, Arango C, Kubilis P, et al: Antibiotic prophylaxis after basilar skull fractures: A meta-analysis. Clin Infect Dis 27:364-369, 1998
- Wormald PJ, McDonogh M: ‘Bath-plug’ technique for the endoscopic management of cerebrospinal fluid leaks. J Laryngol Otol 111:1042-1046, 1997
- Yasargil MG, Fox JL: The microsurgical approach to acoustic neurinomas. Surg Neurol 2:393-398, 1974
- Yerkes SA, Thompson DH, Fisher WS 3rd: Spontaneous cerebrospinal fluid rhinorrhea. Ear Nose Throat J 71:318-320, 1992
- Zlab MK, Moore GF, Daly DT, et al: Cerebrospinal fluid rhinorrhea: A review of the literature. Ear Nose Throat J 71:314-317, 1992