
Meyer’s Loop
Authors
L. Fernando Gonzalez, MD
Kris Smith, MD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
Meyer’s loop constitutes the most anterior extension of the optic radiation in the temporal horn. Patients with intractable epilepsy may undergo temporal lobe surgery, and their optic tract is susceptible to potential injury. Consequently, neurosurgeons must appreciate the surgical implications of this pathway.
Key Words: Meyer’s loop, optic radiation, temporal lobe, vision
Temporal lobe surgery is a common treatment for patients with intractable epilepsy. Different approaches have been used to access the mesial temporal structures. The transcortical-transtemporal approach offers access to the temporal horn and, progressively, to the amygdala and hippocampus. Meyer’s loop constitutes the anteriormost extension of the optic radiation into the temporal horn. This pathway, its correlation with the temporal horn, and its implications for temporal lobe surgery are reviewed.
{kind=link}

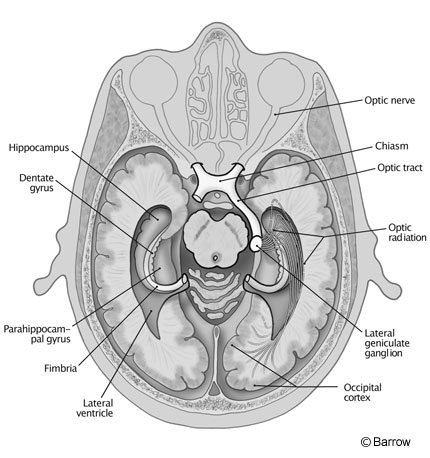
The visual pathway begins at the retina. Ganglion cells converge at the optic disc to form the optic nerve. The nerves enter the cranial cavity through the optic foramina and unite to form the optic chiasm. Fibers from the contralateral (nasal) retina cross to the opposite side at the optic chiasm and join the ipsilateral temporal fibers to form the optic tract. Most of the fibers then synapse at the lateral geniculate body. The last relay of this pathway corresponds to fibers from the lateral geniculate body to the calcarine cortex. These fibers, known as optic radiations, Gratiolet radiations, or the inferior longitudinal fasciculus, constitute the geniculocalcarine tract (Fig. 1). The anterior extension of these fibers in relation to the temporal horn is known as Meyer’s loop.
Based on anatomic and pathological studies from human brain specimens after stroke, Meyer[5] found bundles of fibers from the visual pathway surrounding the anterior aspect of the temporal horn. He also found that the optic radiation was segregated into three bundles on the lateral ventricle: the upper, central, and inferior. The inferior or ventral bundle, known as Meyer’s loop, travels around the temporal horn. This bundle makes a wide anterior and lateral loop around the temporal horn
of the lateral ventricle before curving around the posterior atrium to reach the occipital cortex. These inferior fibers pass into the uncinate region of the temporal lobe and are constituents of the uncinate fascicle located at the limen insula or temporal stem.[2,8,9] At the temporal stem, the middle cerebral artery turns posteriorly and transitions between the sphenoidal or horizontal segment (M1) to the insular (M2) segment.
The upper and central bundles pass through the parietal and high temporal lobes, respectively, to synapse in the primary visual cortex (striate area, Brodmann area 17). The upper fibers carry information from the superior quadrants of the retina; the lower fibers carry information from the inferior quadrants of the retina. The central bundle contains macular fibers (central area of the retina). This anatomical configuration explains superior homonymous quadrantanopia–sparing of central, macular vision after temporal lobe surgery.[1] This defect has been associated with both congruous and incongruous patterns after epilepsy surgery.[8,10,11]
Even using careful anatomical techniques to dissect white matter fibers, however, it can be difficult to isolate the optic radiation from the remaining uncinate fascicle. Based on other anatomic and pathological studies, some authors have questioned the existence of the anterior loop of the optic radiation (Meyer’s loop).[9] Two techniques have been used to investigate the existence of Meyer’s loop.
{kind=link}

The most common method is derived from visual field defects after epilepsy surgery and correlates the extent of resection with the patient’s postoperative deficit. Using different surgical techniques, visual field defects have been found in 52 to 74% of patients after surgery.[3,4,7,10] There is no constant relationship among patients between the size of the temporal lobe excision and the presence or degree of the resulting visual field defect.[4] For example, Tecoma et al.[7] found no significant difference in visual defects in patients undergoing resection of either the temporal dominant or nondominant side although they stated that resections were wider in the nondominant sides. This variability explains why different patients can undergo the same temporal lobe excision, and some develop visual deficits while others do not.
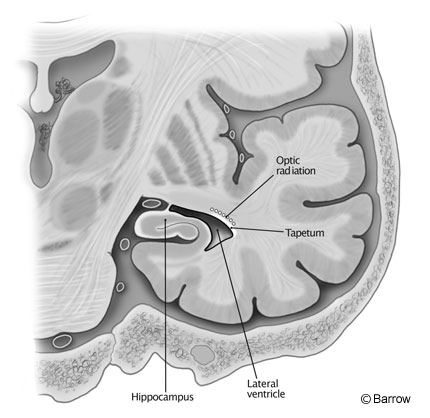
The second method derives from anatomical studies where special techniques are used to isolate fibers (fiber-dissection technique).[9] Using the fiber-dissection technique,[2,9] Ebeling and Reulen[1] studied 50 temporal lobes sectioned coronally at different distances from the tip of the temporal lobe to the occipital cortex. The lateral wall of the temporal horn was composed of a thin layer of corpus callosum, called the tapetum, which separates the ventricular ependyma from the optic radiation (Fig. 2).[6] The optic radiation at the tip of the temporal horn was located in the roof of the ventricle. At the middle aspect of the temporal horn, the optic radiation was found on the roof and lateral wall of the ventricle. At the atrium the optic radiation was found only on the lateral wall of the ventricle. At the atrium, the upper, central, and inferior bundles were present. If these bundles are damaged, the result is complete homonymous hemianopsia. At the occipital horn the optic radiation assumes a horseshoe shape surrounding the lateral wall, floor, and roof of the ventricle.

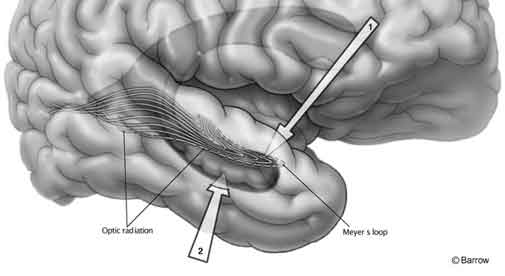
Ebeling and Reulen[1] also found that the mean distance between the anterior tip of the temporal lobe to Meyer’s loop was 27±3.5 mm (Fig. 3). The anterior edge of the loop can be anterior or posterior to the tip of the temporal horn. The mean location was 5mm with a standard deviation of 3.9 mm anterior to the tip of the temporal horn while the anteriormost location was 10 mm anterior to the tip and the posteriormost location was 5 mm posterior to the tip.[1]
{kind=link}

Surgical Implications of Meyer’s Loop
Mesial temporal structures can be accessed through two surgical approaches. With the transcortical approach, the amygdala and hippocampus are reached after the temporal horn is opened through a cortical incision in the second temporal gyrus. Wieser and Yasargil[13] proposed approaching the amygdalohippocampal complex through the transsylvian route (Fig. 4). In this approach, the sylvian fissure is opened and the inferior circular sulcus is exposed. The temporal horn is then opened from its roof, distal to the limen insula or temporal stem. Because the optic radiation is primarily located at the roof of the temporal horn, this approach can be particularly risky in terms of injuring the visual pathway.
A critical point for epilepsy surgeons to recognize is the anterior extension of the optic radiation or Meyer’s loop. Damage to the optic radiation and optic tract can cause similar visual field defects.[8,10] During temporal lobe surgery, opening the choroidal fissure at the level of the temporal horn exposes the ambient cistern. The optic tract, posterior cerebral artery, basal vein of Rosenthal, and anterior choroidal arteries are located in its roof. Resection during temporal lobe surgery should remain inferior to the choroidal fissure and avoid violating the pia-arachnoid membrane to minimize the potential risk to vascular structures and to the optic tract itself, especially during transcortical approaches.[12]
Conclusions
Great variability exists with respect to the position of the anterior extension of the optic radiation in the temporal lobe. Temporal lobe surgery exposes patients to two potential sources of visual field complications: damage to the optic tract in the ambient cistern once the choroidal fissure has been opened and damage to the optic radiation when the temporal horn is opened during transcortical or transsylvian approaches. Resection must remain inferior to the choroidal fissure to protect the optic tract. Because most of the fibers in Meyer’s loop course along the external surface of the temporal horn, the surgical approach to the temporal horn must target the floor or the low lateral wall of the lateral ventricle rather than its roof to preserve this structure.
References
- Ebeling U, Reulen HJ: Neurosurgical topography of the optic radiation in the temporal lobe. Acta Neurochir (Wien) 92:29-36, 1988
- Ebeling U, von Cramon D: Topography of the uncinate fascicle and adjacent temporal fiber tracts. Acta Neurochir (Wien) 115:143-148, 1992
- Jensen I, Seedorff HH: Temporal lobe epilepsy and neuro-ophthalmology. Ophthalmological findings in 74 temporal lobe resected patients. Acta Ophthalmol (Copenh) 54:827-841, 1976
- Marino R, Jr., Rasmussen T: Visual field changes after temporal lobectomy in man. Neurology 18:825-835, 1968
- Meyer A: The connections of the occipital lobes and the present status of the cerebral visual affections. Trans Assoc Am Physicians 22:7-23, 1907
- Rasmussen AT: The extent of recurrent geniculocalcarine fibers (loop of Archambault and Meyer) as demonstrated by gross brain dissection. Anat Record 85:277-284, 1943
- Tecoma ES, Laxer KD, Barbaro NM, et al: Frequency and characteristics of visual field deficits after surgery for mesial temporal sclerosis. Neurology 43:1235-1238, 1993
- Traquair HM: The course of the geniculocalcarine visual path in relation to the temporal lobe. Br J Ophthal 6:251-259, 1922
- Ture U, Yasargil MG, Friedman AH, et al: Fiber dissection technique: Lateral aspect of the brain. Neurosurgery 47:417-426, 2000
- Van Buren JM, Baldwin M: The architecture of the optic radiation in the temporal lobe of man. Brain 81:15-40, 1958
- Wall M: Optic radiations and occipital cortex, in Miller NR, Newman NJ (eds): Walsh and Hoyt’s Clinical Neuro-Ophthalmology. Baltimore: Williams & Wilkins, 1998
- Wen HT, Rhoton AL, Jr., de Oliveira E, et al: Microsurgical anatomy of the temporal lobe: Part 1: Mesial temporal lobe anatomy and its vascular relationships as applied to amygdalohippocampectomy. Neurosurgery 45:549-591, 1999
- Wieser HG, Yasargil MG: Selective amygdalohippocampectomy as a surgical treatment of mesiobasal limbic epilepsy. Surg Neurol 17:445-457, 1982