
Prognostic Utility of Magnetic Resonance Imaging in Traumatic Brain Injury
Authors
Eric M. Horn, MD, PhD
Iman Feiz-Erfan, MD
Timothy R. Harrington, MD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
In the United States traumatic brain injury (TBI) is a serious health issue that significantly affects the health and economy of our society. One of the most important questions confronting clinicians who treat head-injured patients is the level of functional recovery a given patient will attain. Currently, the best early prognosticators are patients’ initial computed tomographic (CT) findings, Glasgow Coma Scale scores, and pupillary responses. These measures are predictive of severe disability or death but offer little information about patients’ long-term cognitive ability. Because it is more sensitive than CT, magnetic resonance (MR) imaging has recently been used to evaluate the extent of TBIs. Thus far, the ability of MR imaging to detect lesions in head-injured patients, especially diffuse axonal injury, is superior to CT. This greater sensitivity, however, has only recently been applied to determine the long-term prognosis of these patients.
Key Words: diffuse axonal injury, computed tomography, magnetic resonance imaging, traumatic brain injury
In the United States the incidence of traumatic brain injury (TBI) is about 1,600,000 per year.[10] About 80% of injuries are mild; the remaining 20% are moderate or severe.[10] Because of the ramifications of the neurological sequelae associated with TBI, clinicians are placed in the unique situation of determining whether treatment is the best course of action. To help make this determination, a clear prognosis is needed during the early stages of injury because delays in treatment can be detrimental to outcome. At present, however, no reliable factors are available to determine the prognosis of these patients.
The best available prognosticators for TBI are limited to patient’s initial Glasgow Coma Scale (GCS) score, the presence of abnormalities on computed tomography (CT), and pupillary responses. Each prognosticator has limited positive predictive value for death, let alone for long-term neurological and cognitive deficits. To help guide treatment for appropriate patients with TBI, a more accurate tool is needed to help determine a patient’s long-term cognitive prognosis. Recent advances in magnetic resonance (MR) imaging technology have improved the ability to diagnose lesions associated with TBI, and this improved imaging sensitivity is being used to help determine prognosis.
Clinical Indicators of Outcome in TBI
The most recent guidelines used to determine the prognosis of severely head-injured patients are based on five separate factors: GCS score, age, pupillary responses, presence of hypotension, and abnormalities on CT.[20] Although these factors are not the only ones used for prognosis, they are the ones most widely used in centers treating patients with TBI.
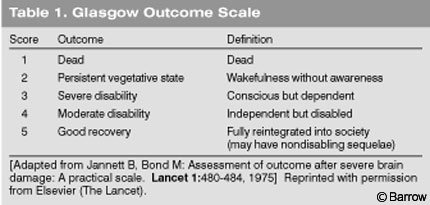
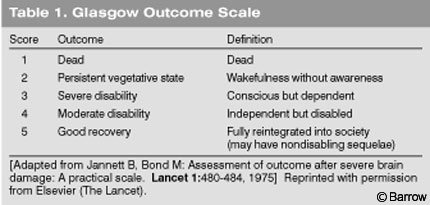
The initial GCS score is inversely correlated with the likelihood of death. In the three largest studies,[3,7,13] an admission GCS score of 3 was associated with mortality rates between 65% and 100%. In contrast, an initial GCS score of 7 was associated with mortality rates ranging from 15% to 27%. Although these data show that the GCS is a strong predictor of death, clinical decisions about the care of patients with TBIs must be made carefully, as evidenced by the same data: 7% of patients with an initial GCS of 3 have a good outcome (Glasgow Outcome Scale [GOS] score of 4 or 5, Table 1).
The age of a patient with a severe head injury at presentation is also inversely related to the likelihood of death. Although the age-related mortality rate associated with a severe head injury (GCS <8) falls on a continuum, the critical threshold appears to be around 50 years. In two large studies, the mortality rate of patients with a severe head injury over the age of 50 years was 78% to 84% while it was 28% to 38% for patients younger than 50 years.[3,15]
{kind=link}
The absence of bilateral pupillary responses after a severe head injury is also correlated with a high mortality rate (91% to 100%).[3,6] A weaker predictive factor is the presence of hypotension after a severe head injury. The mortality rates associated with patients who have periods of hypotension range from 42% to 50% compared to 27% or 28% in normotensive patients.[5,7]
CT and Outcome of TBI
Since the widespread application of CT to the evaluation of head-injured patients, the ability to detect intracerebral abnormalities (e.g., contusions, hematomas) has improved dramatically. The presence of such abnormalities has been used to predict outcome in severely head-injured patients. A common classification scheme includes the presence of mass lesions and diffuse injury and is moderately predictive (positive predictive value of ~75%) of clinical outcome as measured by the GOS.[13] These indicators, however, are still limited as evidenced by the large number of patients who have poor outcomes regardless of their findings on CT. Thus the presence of abnormalities on CT does not appear to add significantly to the predictive value of the clinical variables (e.g., GCS, pupillary responses) used to determine overall outcome in severely head-injured patients.
CT is especially limited in predicting outcome when the findings of a patient with a moderate or severe head injury are normal. In such cases, the negative predictive value is 61% to 76%. Subsequently, however, a large number of these patients have abnormal CT scans. Therefore, early CT scans must be interpreted cautiously.[12,13] The utility of CT in predicting the outcome of moderate or mild head injuries is even more limited because this modality lacks the sensitivity to detect subtle anatomical lesions.
MR Imaging and Outcome of TBI
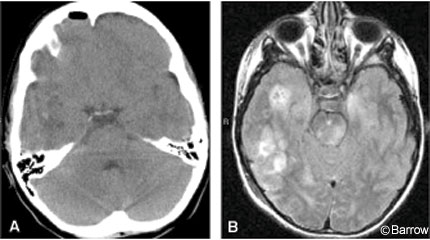
MR imaging is more sensitive than CT for detecting abnormalities in the brain after TBI (Fig. 1).[16] This modality is very sensitive for identifying diffuse axonal injury (DAI) and nonhemorrhagic contusions.[17,22] In one study MR imaging detected DAI in 30% of patients with a mild head injury whose head CTs appeared normal.[14]
In recent years, the use of MRI to assess TBI has increased. However, its use in the early posttraumatic period has been limited because scant evidence of its efficacy is available.
Most studies have had limited success in correlating late MR imaging findings with neuropsychological outcomes.[2,18] One explanation for this limited success is that the functional abnormalities that may be associated with mild, moderate, and severe TBI cannot be defined in terms of standard MR imaging sequences. Although more sensitive than CT, MR imaging still may not reflect functional abnormalities. Notwithstanding, an overall increase in the use of MR imaging has increased appreciation for the extent of structural abnormalities associated with TBI. The main problem now facing neurotrauma clinicians is how to interpret these findings in relation to functional outcome.
MR imaging has been used to determine the prognosis of TBI in various studies.[9] These studies, however, have mostly focused on the technical feasibility of using the modality to detect abnormalities in patients with TBIs. Recently, techniques such as fluid-attenuated inversion-recovery (FLAIR), diffusion-weighting, diffusion tensor, and magnetization transfer imaging have been used to define traumatic lesions.[1,11,19,21] MR spectroscopy also has allowed specific cellular metabolites to be measured after TBI.[4] Functional MR imaging has been used to determine that memory deficiencies associated with TBI correlate with lateralization of activation.[9] These advances in imaging technologies have improved the definition of lesions not detected by conventional CT.
Although MR imaging technology has been used extensively with TBI, a comprehensive analysis of the ability of MR imaging to predict outcomes associated with TBIs has not been performed. A recent study from Greece used MR imaging during the acute phase of trauma (within 48 hours) to predict outcomes in a small cohort of patients. They found that severity of DAI loosely correlated with outcome based on the GOS.[17] However, detailed neuropsychological testing was not used to determine subtle changes in outcome not captured by the GOS. Furthermore, only patients with a normal CT scan were included. Thus, patients with known lesions on CT who may have had unseen secondary lesions were excluded.
Another group in Germany used MR imaging to classify TBI and to predict outcomes. They found that the mortality rate significantly increased as the severity of infratentorial lesions increased.[8] Three to 22 months after injury, GOS scores were significantly worse in patients with severe brainstem lesions. However, the neuropsychological effects of these lesions were not studied. Because MR imaging is more sensitive than CT, a thorough investigation of consecutive patients is needed to correlate MR imaging abnormalities associated with TBI with functional (GOS) and cognitive (neuropsychological) endpoints to identify prognostic factors.
In conclusion, the increased use of MR imaging to evaluate head-injured patients has allowed more subtle intracerebral abnormalities to be detected. This heightened sensitivity for detecting abnormalities is beginning to improve the ability to predict long-term outcomes in patients with TBIs.
References
- Ashikaga R, Araki Y, Ishida O: MRI of head injury using FLAIR. Neuroradiology 39:239-242, 1997
- Azouvi P: Neuroimaging correlates of cognitive and functional outcome after traumatic brain injury. Curr Opin Neurol 13:665-669, 2000
- Braakman R, Gelpke GJ, Habbema JD, et al: Systematic selection of prognostic features in patients with severe head injury. Neurosurgery 6:362-370, 1980
- Cecil KM, Hills EC, Sandel ME, et al: Proton magnetic resonance spectroscopy for detection of axonal injury in the splenium of the corpus callosum of brain-injured patients. J Neurosurg 88:795-801, 1998
- Chesnut RM, Marshall LF, Klauber MR, et al: The role of secondary brain injury in determining outcome from severe head injury. J Trauma 34:216-222, 1993
- Cordobes F, Lobato RD, Rivas JJ, et al: Observations on 82 patients with extradural hematoma. Comparison of results before and after the advent of computerized tomography. J Neurosurg 54:179-186, 1981
- Fearnside MR, Cook RJ, McDougall P, et al: The Westmead Head Injury Project outcome in severe head injury. A comparative analysis of pre- hospital, clinical and CT variables. Br J Neurosurg 7:267-279, 1993
- Firsching R, Woischneck D, Klein S, et al: Classification of severe head injury based on magnetic resonance imaging. Acta Neurochir (Wien) 143:263-271, 2001
- Garnett MR, Cadoux-Hudson TA, Styles P: How useful is magnetic resonance imaging in predicting severity and outcome in traumatic brain injury? Curr Opin Neurol 14:753-757, 2001
- Kraus JF, McArthur DL: Epidemiology of brain injury, in Cooper PR, Golfinos JG (eds): Head Injury, (4th ed). New York: McGraw-Hill, 2000, pp 1-26
- Liu AY, Maldjian JA, Bagley LJ, et al: Traumatic brain injury: Diffusion-weighted MR imaging findings. AJNR Am J Neuroradiol 20:1636-1641, 1999
- Lobato RD, Sarabia R, Rivas JJ, et al: Normal computerized tomography scans in severe head injury. Prognostic and clinical management implications. J Neurosurg 65:784-789, 1986
- Marshall LF, Gautille T, Klauber MR, et al: The outcome of severe closed head injury. J Neurosurg 75 (Suppl):28-36, 1991
- Mittl RL, Grossman RI, Hiehle JF, et al: Prevalence of MR evidence of diffuse axonal injury in patients with mild head injury and normal head CT findings. AJNR Am J Neuroradiol 15:1583- 1589, 1994
- Narayan RK, Greenberg RP, Miller JD, et al: Improved confidence of outcome prediction in severe head injury. A comparative analysis of the clinical examination, multimodality evoked potentials, CT scanning, and intracranial pressure. J Neurosurg 54:751-762, 1981
- Orrison WW, Gentry LR, Stimac GK, et al: Blinded comparison of cranial CT and MR in closed head injury evaluation. AJNR Am J Neuroradiol 15:351-356, 1994
- Paterakis K, Karantanas AH, Komnos A, et al: Outcome of patients with diffuse axonal injury: The significance and prognostic value of MRI in the acute phase. J Trauma 49:1071-1075, 2000
- Pierallini A, Pantano P, Fantozzi LM, et al: Correlation between MRI findings and long-term outcome in patients with severe brain trauma. Neuroradiology 42:860-870, 2000
- Sinson G, Bagley LJ, Cecil KM, et al: Magnetization transfer imaging and proton MR spectroscopy in the evaluation of axonal injury: Correlation with clinical outcome after traumatic brain injury. AJNR Am J Neuroradiol 22:143-151, 2001
- The Brain Trauma Foundation.The American Association of Neurological Surgeons and The Joint Section on Neurotrauma and Critical Care: Management and prognosis of severe traumatic brain injury. J Neurotrauma 17:449-628, 2000
- Wild JM, Macmillan CS, Wardlaw JM, et al: 1H spectroscopic imaging of acute head injury—evidence of diffuse axonal injury. MAGMA 8:109-115, 1999
- Yokota H, Kurokawa A, Otsuka T, et al: Significance of magnetic resonance imaging in acute head injury. J Trauma 31:351-357, 1991