
Wechsler IQ, Hong Kong List Learning Test, and the BNI Screen for Higher Cerebral Functions
Authors
Florence D. M. Lai, MPhil
George P. Prigatano, PhD*
Clinical Psychology Department, Kowloon Hospital, Hong Kong
*Division of Neurology, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
Eighty-five Cantonese-speaking brain dysfunctional patients were administered a Cantonese version of the BNI Screen (BNIS) for Higher Cerebral Functions. They were also administered the Wechsler Adult Intelligence Scale—Revised Form (WAIS-R) and the Hong Kong List Learning Test (HKLLT). The BNIS Total score correlated 0.69 with Full-Scale IQ, and the HKLLT correlated 0.51 with the delayed verbal recall total score from the BNIS. These findings suggest that this adapted version of the BNIS can be used to assess higher cerebral functions in Cantonese-speaking populations.
Key Words: BNI Screen, brain injury, higher cerebral functions, neuropsychological testing
Prigatano and Palencia[3] attempted to extend the construct and concurrent validity of the BNI Screen (BNIS) for Higher Cerebral Functions by specifically correlating the Total score on the BNIS with the Halstead Impairment Index (HII) score[4] and the IQ scores obtained from the Wechsler Adult Intelligence Scale-Revised (WAIS-R) Form.[6] Correlations of .50 to .60 were obtained, supporting the proposition that the BNIS is a valid neuropsychological measure. The present study attempted to partially replicate these findings using a Cantonese-speaking population in Hong Kong.
The Speech and Language subtests were translated into Cantonese. The item used to stimulate spontaneous affect was also changed to account for cultural differences between the Hong Kong population and the American population in which this test was standardized. This type of translation is similar to that reported in a German translation of the BNIS (See Reliability and Validity Studies for the German Adaptation of the BNI Screen for Higher Cerebral Functions in this issue).
The relationship between the BNIS Total score and various subtest scores on a Cantonese translation of the WAIS-R was calculated. The Hong Kong List Learning Test (HKLLT)[1] also was included to assess whether the delayed verbal memory score on the BNIS correlates with performance on this test. In this way, an attempt was made to expand the previous validation study conducted by Prigatano and Palencia.[3]
Four hypotheses were studied. (1) The BNIS Total score would significantly correlate positively with the Full-Scale WAIS-R IQ. (2) The BNIS Speech and Language score would significantly correlate positively with the Verbal IQ. (3) The BNIS Visuospatial score would significantly correlate positively with the Performance IQ. (4) The verbal delayed recall score (i.e., recalling three words with distraction) on the BNIS would correlate positively with a 10-minute delayed recall on the HKLLT.
Materials and Methods
Subjects
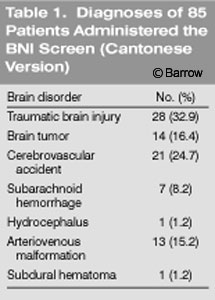
Eighty-five patients (61 males, 24 females; mean age, 43.5 years; range, 11 to 69 years; standard deviation (SD)=13.3) with documented brain disorders (Table 1) were transferred to our hospital from an acute hospital. Their mean numbers of years of education was 9.5 (range, 0 to 18 years; SD=3.9). The mean chronicity (time from onset of brain disorder to testing) was 17 months (range, 1 to 132 months, SD=17). The inclusion criteria for the study were as follows: (1) a medically documented brain disorder, (2) complete neuropsychological test protocols, (3) no history of psychiatric disturbance, and (4) able to read and write in Cantonese.
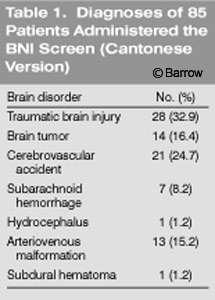{kind=link}
Procedures
The WAIS-R and HKLLT were administered according to standardized procedures. The WAIS-R consists of 11 subtests, which are used to derive a Verbal IQ and Performance IQ. These two composite scores are combined to calculate the Full-Scale IQ. The HKLLT consists of two different lists of 16 Chinese words, all of which are two-character nouns. Thirty minutes are required to administer the verbal learning, 10-minute and 20-minute delayed recall tests, and recognition tests.
Like the original BNIS, the Cantonese version of the BNIS consists of a set of plastic cards, record form, and standard stopwatch. The test requires 10 to 25 minutes to administer. High scores suggest less impaired cognitive functioning than low scores. Subtest scores indicate patients’ performance in each cognitive domain. A total score of less than 47 from the possible 50 points suggested the possible presence of cognitive deficits in an American population.[2]
All neuropsychological tests were administered by the first author. All patients were given the BNIS (Cantonese version) first, followed by the HKLLT and WAIS-R, respectively.
Data Analysis
All statistical analyses were performed with Statistical Package for the Social Sciences–10.1 for Windows. Descriptive statistics were calculated. Pearson correlation coefficients were calculated for the WAIS-R Full-Scale IQ and BNIS Total scores. The scores on the Speech and Language and Visuospatial subtests of the BNIS were correlated with WAIS-R Verbal IQ and Performance IQ. The BNIS score for the three verbal delayed items were correlated with the 10-minute delayed recall subtest of the HKLLT.
Results
Correlations of BNIS Total Score with WAIS-R IQ Scores
The correlation between the BNIS Total score and the WAIS-R Full- Scale IQ was 0.69 (p<.01). In two independent groups of brain dysfunctional patients, Prigatano and Palencia[3] reported correlations of .58 (p<0.1) and .53 (p<.01). Thus, the correlation obtained from the Hong Kong population is of the same magnitude and direction as reported in the American population, supporting the first hypothesis. It is important to note that the magnitude of the correlations has remained the same across these two different cultures using three different samples of brain dysfunctional patients.
Table 2 provides a correlational matrix between three subtests on the BNIS and the WAIS-R IQ measures and measures obtained from the HKLLT. The correlation of the BNIS Speech and Language subtest and the Verbal IQ was 0.48 (p<.01). The findings were comparable to the correlation of .56 and .47 found in two independent groups of American brain dysfunctional patients.[3]
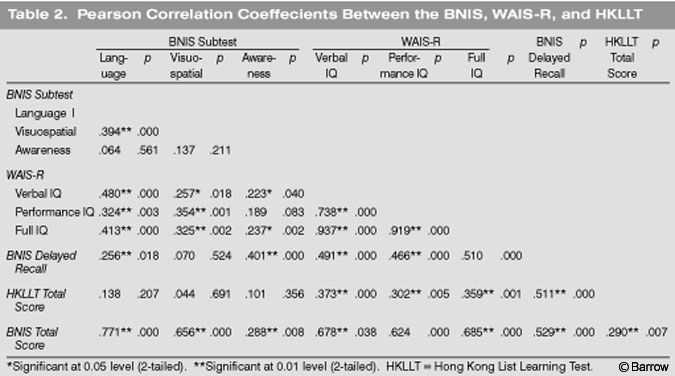{kind=link}
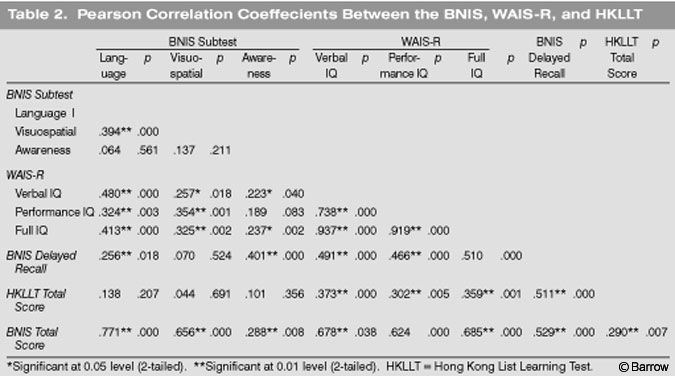
The correlation between the BNIS Visuospatial score and Performance IQ was 0.35 (p<.01). This magnitude of correlation was reported by Prigatano and Palencia,[3] again in two independent groups of brain dysfunctional patients. In their study, correlations were .47 and 41, respectively, supporting Hypotheses 2 and 3.
The correlation between the recall of three words (verbal delayed recall score) on the BNIS and the 10-minute delayed-recall score and the HKLLT was at 0.51 (p<.01).
Prigatano and Palencia[3] reported that the correlation between the WAIS Full-Scale IQ and the awareness measure on the BNIS produced a nonsignificant correlation for one group of dysfunctional patients (r =0.08) and a correlation of .36 (p=.05) in another group. It was noted that the severity of brain injury might account for these different correlations as well as time since injury when the patient was examined. The correlation obtained in the Hong Kong population fell between these two extremes (r =.237).
Discussion
The present data replicate and expand the observations by Prigatano and Palencia[3] using a Cantonese-speaking Hong Kong population. The BNIS Total score was found to significantly and positively correlate with the WAIS-R Full-Scale IQ. Other investigators have reported the same phenomenon.[5]
The BNIS Speech and Language subtest correlated significantly with the WAIS-R Verbal IQ. The correlation between the BNIS Visuospatial score and the Performance IQ was also significant. Collectively, these findings suggest that the BNIS shows good construct and concurrent validity across cultures.
The BNIS is “user friendly.” It is easily administered and requires only 10 to 25 minutes to complete. The test materials can be transported easily and are therefore convenient for bedside neuropsychological assessment. It also can be administered repetitively to document changes in patients’ functioning over a brief period of time.
The persistent problem of impaired awareness after brain injury is further highlighted by the present test findings. Having patients predict their performance on a memory test is, of course, one possible indirect measure of awareness. Yet, in this study, as well as in the Prigatano and Palencia study,[3] no correlations were found between this ability and performance on measures of intelligence. This finding does not mean that awareness is independent of intelligence. Rather, it indicates that awareness is a complicated function that cannot easily be measured by standard IQ tests.
Conclusion
The correlations between the BNIS Total score and the WAIS-R Full-Scale IQ, the BNIS Speech and Language score and Verbal IQ, the BNIS Visuospatial score and Performance IQ, and the BNIS verbal delayed recall score and the delayed recall tests of the HKLLT were all positive and significant. These findings suggest that the BNIS is a useful screening tool to assess higher cerebral functions in clinical practice and for future research on brain dysfunction in Cantonese speaking populations.
References
- Anges S, Kwok I: Hong Kong List Learning Test. Hong Kong: The Chinese University of Hong Kong, 1999
- Prigatano GP, Amin K, Rosenstein LD: Manual for the BNI Screen for Higher Cerebral Functions. Phoenix, Arizona: Barrow Neurological Institute, 1995
- Prigatano GP, Palencia B: Halstead Impairment Index Score, Wechsler IQ, and the BNI Screen for Higher Cerebral Functions. BNI Quarterly 16(3):22-27, 2000
- Reitan RM: Manual for Administration of Neuropsychological Test Batteries for Adults and Children. Tucson, Arizona: Reitan Neuropsychology Laboratories, 1955
- Wass PJ: An analysis of the construct-related and ecological validity of the Barrow Neurological Institute Screen for Higher Cerebral Functions (dissertation). Windsor, Ontario, Canada: University of Windsor, 1997
- Wechsler D: Wechsler Adult Intelligence Scale-Revised. San Antonio, Texas: The Psychological Corporation, 1981