
Cessation of Hallucinations After Endoscopic Third Ventriculostomy: Case Report
George P. Prigatano, PhD
Heather Caples, PhD
Harold L. Rekate, MD*
Divisions of Neurology and *Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
A 48-year-old, right-handed woman with hydrocephalus related to a Dandy-Walker malformation complained of memory difficulties and auditory and visual hallucinations. After undergoing a third ventriculostomy, she reported complete cessation of the hallucinations. Memory impairment persisted. The psychiatric literature documents that third ventricular enlargement can be associated with “first episode psychosis.” This case report suggests that reduction in the size of the third ventricle may be associated with cessation of hallucinations in some patients. No theoretical model has emerged to explain these findings.
Key Words: Dandy-Walker syndrome, hydrocephalus, neuropsychological test scores, psychosis
Abbreviations used: CT, computed tomography; MMPI-2, Minnesota Multiphasic Personality Inventory-Form 2
Historically, neurologically based visual or auditory hallucinations have been attributed to cortical disturbances involving the temporal lobes, occipital lobes, or both.[2] Neuroimaging studies reviewed by Lishman[8] suggest that activation of Broca’s area is implicated in auditory hallucinations. However, no single area of the brain could be unequivocally associated with auditory or visual hallucinations. Both cortical and subcortical structures have been implicated during schizophrenic hallucinations.[8] Alteration of hallucinations by pharmacological or surgical treatment may provide clues about the underlying cause of the hallucinatory experiences. We report a patient who suffered hallucinations related to a Dandy-Walker malformation. After undergoing an endoscopic third ventriculostomy, her hallucinations resolved.
Case Report
History
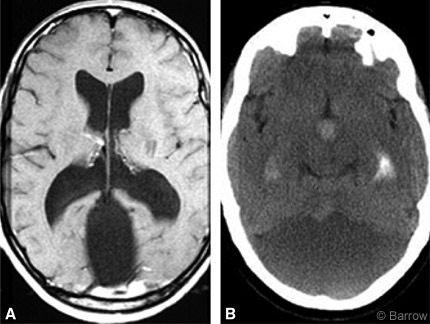
A 48-year-old, right-handed woman was referred by her neurologist for neurosurgical treatment of a recently discovered Dandy-Walker malformation associated with dilatation of her third and lateral ventricles (Fig. 1). She sought neurologic care for headaches thought to be migraines, visual scintillations, deteriorating memory, and clumsiness. Her problems had been known since she was about 2 years old. As a toddler, her motor development was slow and she did not walk until she was 2 years old. She had been considered a clumsy child and had been teased about her lack of athleticism. In her early 20s, she noted occasional diplopia and significant difficulties with memory. However, she completed nursing school and worked as a registered nurse in extended care facilities for many years. In adulthood, her headaches continued to worsen; they were intermittent and mostly refractory to standard medical regimens. Recently, her headaches had improved after she took Depakote (Abbott Laboratories, Abbott Park, Illinois).
Physical Examination
Upon physical examination, her head circumference was 58.5 cm, about 1.5 cm above the 95th percentile. Otherwise, her general physical examination was normal. She had no overt abnormalities on neurologic examination. Despite complaints of intermittent diplopia during the examination, no abnormalities of eye movements were observed.
Diagnostic Imaging
Magnetic resonance imaging showed a large cyst in the posterior fossa. An elevated torcula herophili and agenesis of the cerebellar vermis were consistent with a Dandy-Walker malformation. Supratentorially, her third and lateral ventricles were enlarged. Her corpus callosum was intact (Fig. 1).
Treatment
Hydrocephalus related to a Dandy-Walker malformation with recent decompensation was diagnosed. The patient was given a choice of shunt placement or endoscopic management. She elected to attempt to continue life without a shunt. Initially, a ventricular access device was placed so that intracranial pressure could be monitored and dye injected to determine whether the ventricular system communicated with the Dandy-Walker cyst. After the device was inserted, iohexol 180 (10 cc) was injected through the reservoir. The dye quickly flowed into the fourth ventricular cyst. Since flow between the third ventricle and the encysted fourth ventricle was unimpeded, the patient was considered a candidate for an endoscopic third ventriculostomy.
In this procedure, the endoscope is inserted into the right lateral ventricle through a right frontal bur hole and then advanced into the third ventricle. Under direct vision the floor of the third ventricle is perforated, creating an internal bypass between the third ventricle and the cortical subarachnoid space. The obstruction at the outlet foramina of the fourth ventricle is thereby bypassed. The procedure was performed uneventfully, and the patient was discharged from the hospital. At follow-up visits 3 and 12 months after surgery, she was doing well. She had no headaches, and her coordination and mood had improved markedly.
Neuropsychological Test Findings and Self-Reports
The patient underwent a neuropsychological evaluation 2 weeks before and 6 months after the third ventriculostomy. Initially, she reported being separated from her second husband and experiencing considerable emotional distress. She noted, however, that she had longstanding adjustment difficulties. She described “disruptive behavior” in school and then at work for several years before surgery. She stated that she had frequently been reprimanded for being argumentative, insistent, and controlling.
She reported long-term memory problems that had interfered with her work, but she was able to compensate for them adequately. More recently, however, she had experienced both auditory and visual hallucinations. She could not state precisely when the hallucinations had begun to occur, but she noted that she had been experiencing them for “some period of time.” She related this information calmly. She indicated that she frequently heard someone calling her name. She frequently saw individuals reaching into a drawer at her home even though she knew no one was there. After further questioning, she indicated that the visual hallucinations occurred more frequently on the left side of space than on the right side of space.
She described her vision as often “blurry.” She may have experienced diplopia. She indicated that she had frequent headaches, but they had improved with medication.
Table 1 lists the patient’s neuropsychological test scores before and after surgery. On the BNI Screen for Higher Cerebral Functions,[10] her scores improved modestly after surgery, particularly on memory subtests. Before surgery her total score converted to a T score was 41; afterward, it was 58. This difference is clinically significant. Verbal fluency, as measured by the Controlled Oral Word Association subtest of the Multilingual Aphasia Examination,[7] was below average on both examinations.
On the Trail Making Test, Parts A and B,[12] a test thought to sample visual scanning and the ability to shift cognitive set rapidly, her performance was in the low average range before and after surgery.
On the Wechsler Adult Intelligence Scale, third edition,[7] her IQ values were in the average range before and after surgery. Despite her memory complaints, she performed normally on several memory tasks before and after surgery. However, her visuospatial memory was poor on both examinations (see Brief Visuospatial Memory Test scores, Table 1).
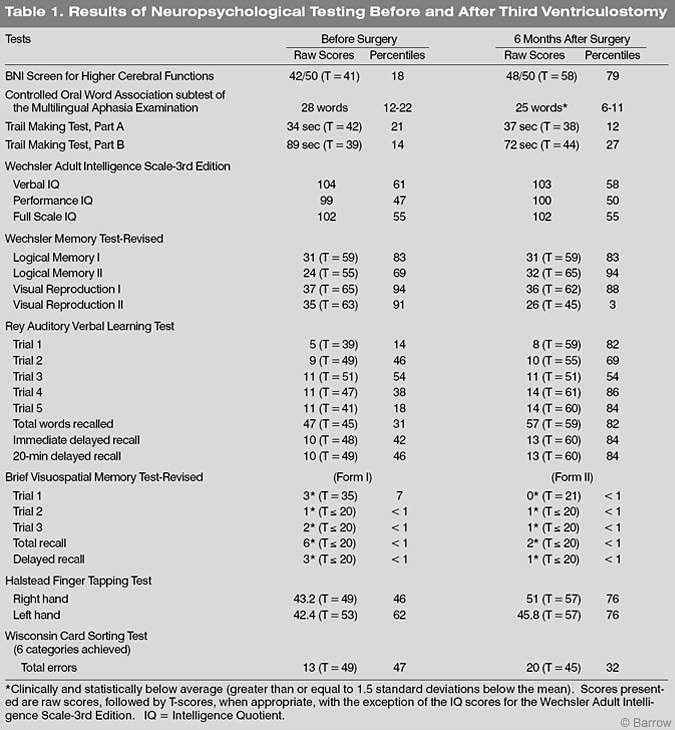
Her performance on verbal memory tasks improved modestly (Rey Auditory Verbal Learning Test and the Logical Memory Subtest of Wechsler Memory Scale-Revised Form).[7] Her postoperative speed of finger-tapping with her right hand on the Halstead Finger Tapping Test 12 improved compared to her preoperative test scores.
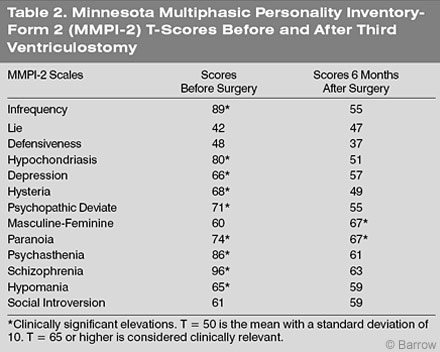
Her self-reported psychiatric status improved dramatically after surgery (MMPI-2; Table 2). Her scores on the scale thought to reflect possible psychotic thought processes (namely, the schizophrenia scale) decreased substantially. She complained considerably less about her physical functioning, and she reported approaching social rules in an acceptable manner.
Not captured in these test findings is her manner of presentation. On both occasions, she spoke loudly and was disinhibited. While speaking to her, one could detect no notable change. However, she was adamant that her memory problems persisted although they had improved mildly and that her hallucinations had ceased entirely. Her findings on the neuropsychological tests and on the MMPI-2 tend to support these clinical observations. The question arises, however, why would a third ventriculostomy dramatically improve her selfreport of hallucinations?
Discussion
This case study is unusual because the patient reported abrupt cessation of hallucinations after a third ventriculostomy that reduced the size of her enlarged lateral and third ventricles. No theoretical model is available to explain these findings. However, clinical reports have related posterior fossa lesions to psychotic behavior.[9,13] Neuroimaging studies have shown enlarged ventricles and cortical atrophy in some, but not all, schizophrenic patients.[8] After reviewing the literature, Raz and Raz[11] concluded that ventriculomegaly was reliably observed in schizophrenic patients and that increased volume of the lateral and third ventricles was related to the severity of illness in this population.[1] Studies of patients with “first-episode” psychosis have reported structural brain abnormalities throughout the cortex and have repeatedly mentioned enlargement of the lateral and third ventricles.[5,6] In particular, the size of the third ventricle has correlated with persistent auditory hallucinations in patients with schizophrenia.[4] Developmental delay also may be related to significantly enlarged third and lateral ventricles.[3]
The third ventricle is “bound by the anterior commissure, the fornix, the stria medullaris, the pineal body, the superior and inferior colliculi, the midbrain and mamillary body, the thalamus, and the hypothalamus.”[5] The thalamus, which is a key structure for all sensory representation, projects to multiple cortical regions, enabling visual and auditory perception. Traditionally, visual and auditory hallucinations have been related to cortical disturbances, particularly involving the temporal lobe.[3] However, altering thalamic input to cortical regions could conceivably produce hallucinatory experiences. In our patient, placement of the third ventriculostomy may have improved thalamic functioning indirectly.
Conceivably, any intervention that would disrupt thalamic function might increase psychiatric symptomatology. Recently, a patient showed significant psychiatric complications, including impulsiveness, aggressiveness, and what was described as “an organic personality disorder,” after undergoing a third ventriculostomy.[1] Therefore, a third ventriculostomy might produce different outcomes, depending on the degree to which the thalamus and related structures are affected by the procedure. This hypothesis needs to be explored further. Given the numerous reports that the size of the third ventricle appears to be related to disturbances such as developmental delay and psychotic features, this region should be especially fruitful for interdisciplinary investigation of the emergence and cessation of hallucinations.