
The Art and Science of Milieu-Oriented Neurorehabilitation*
Pamela S. Klonoff, PhD
Division of Neurology, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
*This article is based on a lecture given in November 2002 as part of the Grand Rounds series at Barrow Neurological Institute named the Lage Lectureship in honor of Gustavo Lage, MD (1926-2002).
This paper was written as a tribute to Gustavo Lage, M.D. (1926-2002) who inspired the incorporation of self-psychology principles into the psychotherapy of patients with brain injuries at the CTN. This article describes the role of self object relationships, catastrophic reactions, and empathic responsiveness in milieu-oriented psychotherapy. Samples of the art and poetry of two program participants illustrate their personal experiences of their brain tumors. A review of prior outcome research demonstrates the efficacy and enduring benefits of milieu-oriented treatment for as long as 11 years after discharge.
Key Words: catastrophic reaction, neurorehabilitation, traumatic brain injury
Abbreviations used: CTN, Center for Transitional Neurorehabilitation; ADHNR, Adult Day Hospital for Neurological Rehabilitation
This article is divided into three parts. First, drawing on the teachings of Dr. Gustavo Lage, Heinz Kohut, Ernest Wolf, and other self-psychologists, the underpinnings of self-psychology and their application to our milieu-oriented rehabilitation program at the CTN are reviewed. Second, artistic and creative products from work with two CTN patients, whom I believe were partially inspired by their personal experience of their brain injuries and by participation in a milieu-environment, are presented. Finally, outcome research on the efficacy of our work in helping patients maintain productive work and school as long as 11 years after discharge from the program is reviewed.
The Developmental Process
Self-psychology has been defined as the “psychology of the vicissitudes of the self–its emergence and development, cohesion, boundaries, structure, functions and disorders.”[21] Central to the understanding of self-psychology is the concept of self-objects. A self object is an object or person who in the real world is separate and distinct, but who in the psychic world is experienced as part of the self, because that object or person performs certain functions for the self, like soothing, calming and organizing.[12,15] Self-object experiences are integral to the emergence, maintenance, and completion of the self.[21] The self-object relationship refers to an intrapsychic experience. 21 Parents are the earliest and most important self-objects; as individuals grow, others function as self-objects, including grandparents, teachers and friends. Self-objects are needed throughout our life. With maturation the selfobjects evolve from primitive to mature, from the need for the physical presence to symbolic representation (e.g., art, literature, music, ideas, religion, and scientific accomplishments).[12,21]
The concept of self-cohesion is central to self-psychology and is highly relevant to the process of neurorehabilitation. Self-cohesion is comparable to ego strength. It allows individuals to tolerate stresses, to remain emotionally stable, and to experience a state of well being and self-esteem.[14,21] Empathic responses from significant self-objects during early childhood are critical for the development of self-cohesion.[12] Individuals who are deprived of self-sustaining self-object experiences may undergo fragmentation, or instability and disintegration of the self.[21] In a state of fragmentation, these individuals experience apprehensiveness, low energy, moodiness, poor focus, and disorganization of the self. It is as if the structure of the self breaks into component fragments.[21]
There are three lines of the development of the self. In early childhood the grandiose self manifests itself through grandiosity and exhibitionism. It matures through empathic mirroring of appropriate self-objects, usually the parents. With “good enough parenting,” the intensity of the grandiose self is diminished; experiencing optimal frustrations teaches children their limits.[1] Children develop self-esteem based on the level of acceptance (or rejection) and approval (or disapproval) that they receive. It is as if the parents’ eyes are the mirror in which children perceive themselves. The self-object needs of developing children must mature from archaic demands for perfection and constant attention to self-esteem with a healthy self-object need for occasional praise and recognition.1 In adolescence the grandiose self is the creator of ambitions, strivings for power and success, and attempts toward enjoyment.
The idealized parental imago (an omnipotent object, usually the parent, whom the child idealizes) gradually matures into a set of ego ideals and into a set of tension-regulating structures through the child’s merger with the omnipotent objects’ image of calmness, infallibility, and omnipotence. As the child matures, the need to idealize alters from the wish to merge with others to knowing that friends and family are available when needed.
Alter-ego or twinship needs manifest in childhood as the need to feel like a human among other humans. With maturation, this need manifests in the form of peer relationships, teammanship, and so on.[14] Therefore, the self consists of three major constituents: the pole of ambitions, the pole of ideals, and the intermediate area of talents and skills.[12]
A healthy self necessitates a sufficient self-object environment during childhood. The healthy self internally regulates self-esteem, calming and soothing the self.[1] However, individuals who experience significant empathic failures and narcissistic injury undergo a loss of cohesion and fragmentation resulting in feelings of emptiness, depression, anxiety, or worthlessness.[14,21] A weak self develops from faulty selfobject experiences.[21] Major empathic failures by self-objects result in the enduring presence of an archaic grandiose self, a need for idealized omnipotent objects with which to merge, or a need for a twin or alter-ego self-objects. When patients enter treatment, the archaic struggles are reactivated.[14] The therapeutic process is based on transferences, which are the fears, defenses, and distortions caused by early trauma to the self, that then re-emerge in relations with others later in life when they are no longer appropriate.[21]
Narcissistic Rage and Catastrophic Reactions
Injured self-esteem can result in the experience of narcissistic rage. It is caused by the frustration of the omnipotence of the grandiose self when there is interference with the experience of absolute perfection of the archaic self.[19] The rage becomes directed toward external objects perceived to be the cause of a narcissistic insult. In actuality, it is the reaction of the self when it experiences a sense of shame, vulnerability, helplessness, and loss of integrity. Kohut described the feelings that the self experiences after narcissistic insult as “disintegration anxiety.”[1] It is described as a sense of loss of self, humanness, or wholeness.[4] The common element of all forms of narcissistic rage is the need to “right a wrong, and undo a hurt by whatever means.”[13] Narcissistic rage can also result in a series of self-destructive behaviors, including the use of drugs and self-mutilation. At times, the feelings of emptiness, disillusionment, fragility, and shame can be so intense that individuals feel no recourse except suicide. In this way, individuals wipe out the offending, disappointing reality of being damaged.[11]
There are parallels between narcissistic rage as defined by Kohut and “catastrophic reactions” as described by Goldstein in 1952.[2] Catastrophic reactions occur after brain injury, when individuals can no longer accomplish tasks that were easily accomplished before injury. Goldstein identified “anxiety” or the “threat to self-realization” as the underlying reason for the catastrophic reactions. Both formulations are based on the recognition of the damaging effect that perceived failure has on the integrity of the self.[6] Therefore, both formulations are forms of fragmentation and focus on the effect of failures of self-esteem. Individuals then experience intense anxiety and shame related to their perceived defects. Rage becomes the response to the injury to the sense of self.[4]
Acquired brain injury represents a serious threat to self-esteem even for emotionally healthy individuals. Therefore, patients in the milieu setting often manifest catastrophic reactions. As their awareness and appreciation of their postinjury limitations increase, they often develop an intense reaction to the realization of their incapacities. This assault on their sense of self often leads to periods of helplessness, hopelessness, and depression.
Treatment Considerations
Empathic understanding by the therapist represents an attempt to experience the situations of patients and to use that knowledge to understand patients’ reactions. In this “subjective listening mode,”[17] the psychotherapist “listens as best as possible to what patients communicate, limiting one’s own inferences or preconceptions.”[17] The therapist attempts to understand the subjective experience of patients by entering into their reality.[21] The therapist thereby uses “vicarious introspection” to sense himself or herself into the experience of patients.[12,21] The therapist has “the capacity to think and feel himself into the inner life of another person.”[12] The atmosphere created is one of support, acceptance, and nurturance.
The therapist provides a therapeutic environment, also referred to as the holding environment[20] or “accepting analytic ambience.”[21] Patients feel supported, understood, and significant because of the “empathic resonance” with the therapist.[12] The therapist’s calmness, optimism, and analytic exploration enable patients to experience increased feelings of well being.[14,21] The therapist’s empathic responsiveness enables patients to feel that the therapist understands what they think and feel. Empathy is synonymous with “affect attunement.”[18]
The reactivation of archaic struggles results in three types of self-object transferences with the therapist: mirror transference, in which patients seek accepting, admiring, and approving mirroring; idealizing transference, in which the therapist is idealized with a merger with calmness, wisdom, and strength; and the twinship or alter-ego transference, in which the therapist is perceived as similar to patients in terms of appearance, manner, outlook, and opinion,[21] thereby affirming the experiences of patients. [14] In the therapeutic process the transference manifestations occur within the damaged self, increasing cohesion and harmony of the self. The self is strengthened by the psychoanalytic process, through a disruption-restoration process.[1,21]
In the developmental process, tension regulation results from interactions between the self and self-object. Through the process of transmuting internalizations, children acquire the structuralization that permits them to regulate tension by themselves by internalizing parts of the important self-objects.[1,14] As part of developing healthy self-object processes, self-object failures, resulting from faulty empathic responses, occur within the therapeutic relationship (e.g., erroneous, ill-timed interpretations). Patients work through the process of disruption by transmuting internalization. These “optimal failures” serve to strengthen the psychological resiliency of patients.[12] Treatment becomes successful because patients reactivate the needs thwarted in childhood, through replication of an old injury.[17] Through the process of optimal frustrations, patients acquire the ability to sustain themselves with self-object resources in their adult world.[12]
“Given the proper therapeutic ambience, understanding, knowledge, and self-expansion will occur in the therapy.” [14] The therapist acts as an alter ego, helping patients with planning and healthy decision making, guiding and regulating their behavior toward attainable goals. The therapeutic effect is derived by the therapist understanding and explaining interpretations of the patients’ inner life.[12] This process is essential for patients with frontal lobe damage, whose deficits in executive functions may impede their ability to reason, plan, or problem solve in their own best interest.[5]
An important role of the psychotherapist working with patients with brain injuries is to perceive, understand, and educate patients about their type of catastrophic reaction. Forms of the catastrophic reaction typically observed in the treatment environment include sadness, frustration, anxiety, shame, and despair. Other manifestations include emotional withdrawal, intense rage, disavowal, and concealment.6 Recognizing that the catastrophic reaction is an expression of anxiety and shame is itself an empathic response. Educating and helping patients make the necessary modifications in their environment, goals, and ambitions become integral in helping them to avoid catastrophic reactions.[6]
Often after brain injury, the therapist helps patients to avoid risk-taking and self-destructive behavior, patterns that were in evidence before the injury, patterns that often resulted in the brain injury in the first place. The therapeutic process requires patients to better understand the causes of their behavior. It enables patients to learn to cope with their psychic pain; therapy cannot relieve it. The curative aspect of treatment emerges as patients learn to find mature self-objects so that they can achieve a narcissistic balance.[14,21] They develop an observing ego and can undertake the processes of self-reflection and self-control.
{kind=link}
The healing contribution of the milieu environment is evidenced by patients’ intensive exposure to an empathic setting, where they experience compassion, caring, and the availability of multiple staff 4 to 5 days a week for several months.[17] The therapists’ presence provides patients with feelings of security and reassurance, where their limitations are accepted and understood.[4]
Patients participating in the milieu program focus on restoring functional independence, meaning, and productivity in their lives.[9,16] Group treatment counteracts feelings of alienation and isolation.[5] Patients often find it validating to recognize that other individuals, while overwhelmed and discouraged like themselves, are learning to cope and adapt to their limitations.[6]
Families are active participants in the milieu neurorehabilitation process so that they can reestablish healthy self-object relationships with the patients. Family members often require intensive psychotherapy to cope with their damaged or imperfect loved one. Many families experience their own form of narcissistic injury when they recognize that they cannot reverse the extent or severity of their loved one’s deficits.[4] Empathic responsiveness to the family enables them to work through their personal reactions of sadness, guilt, and despair.
Termination of therapy is often characterized by patients developing selfanalytic skills combined with mobilization of creative activities and increasing ease and satisfaction in social relationships.[21] Kohut[10] defined “transformed narcissism” as “creativity, empathy, a capacity to tolerate one’s own impermanence, a sense of humor and wisdom.”[21] With increased cohesion, patients with brain injuries reintegrate into the milieu of their community, explore areas of creativity and interest, and control undesirable or self-destructive behavior.[4] Therapists assist patients in their quest for self-reinvention[3] as they establish new identities, roles, purposes, and challenges. It is hoped that they also find others in their environment who understand and accept their limitations and who can provide an enduring empathic self-object experience.
Illustrative Cases
The following two case studies represent the application of many of the preceding concepts to the psychotherapy of two patients. Both patients had brain tumors and participated in intensive psychotherapy. Both used creative outlets to express and struggle with their neurological changes and decline.
Case 1
At the age of 47, a physician was diagnosed with a low-grade ependymoma of the fourth ventricle. His postoperative deficits included dysarthria, swallowing, balance, gait, stamina, double vision, hand dexterity, and coordination. He attended the CTN program from May 1995 until February 1996. He received Speech and Language Therapy, Physical Therapy, and Occupational Therapy. Initially, he was reticent about psychotherapy, but he gradually developed a sufficient working alliance with the team to embrace Individual and Group Psychotherapy. His wife was highly committed to her husband’s recovery and rehabilitation and actively participated in the milieu treatment process.
In September 1995 the patient began a gradual and part-time return to his medical practice. His initial tasks included chart review, committee meetings, and patient care. He gradually increased his work hours and responsibilities until he was re-integrated at work. In January 1997, he died from complications related to central sleep apnea.
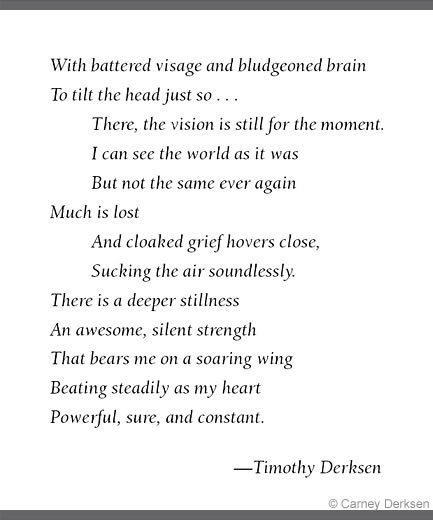
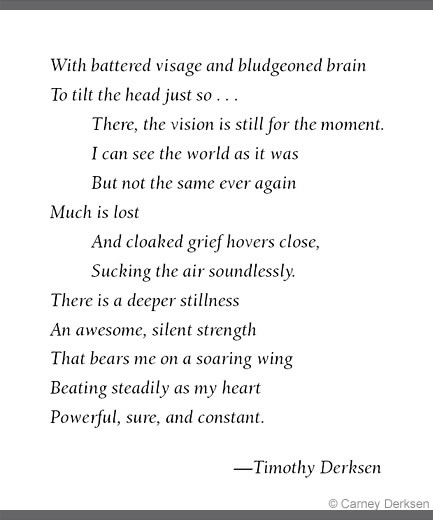
After his surgery the patient began to write poetry, which he shared during his Individual Psychotherapy sessions. The poems depicted his personal struggles after surgery. In the first poem (Fig. 1), the patient reflected on his own deficits, referencing “battered visage” as his cranial nerve damage and his diplopia as “to tilt the head just so . . . There the vision is still for the moment.” His realization that “I can see the world as it was; But not the same ever again” reflects the feelings of the narcissistic injury and catastrophic reactions caused by the changes in his capabilities. “Much is lost,” reflects the fragmentation process. His struggle between combating feelings of depression, “And cloaked grief hovers close,” alternates with the quest for hope “An awesome, silent strength; That bears me on a soaring wing.”
{kind=link}
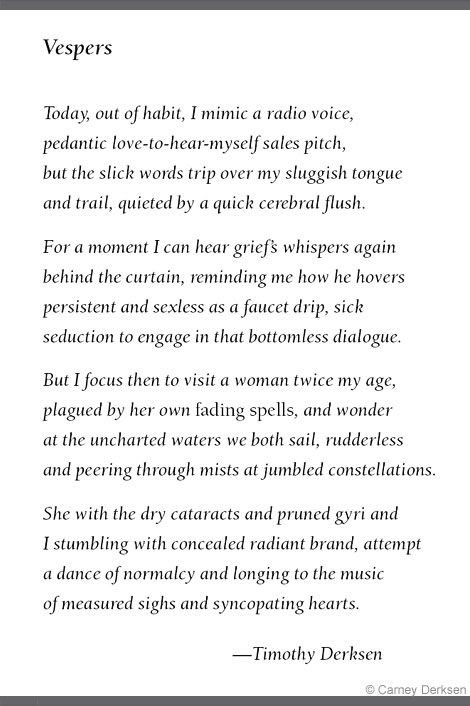
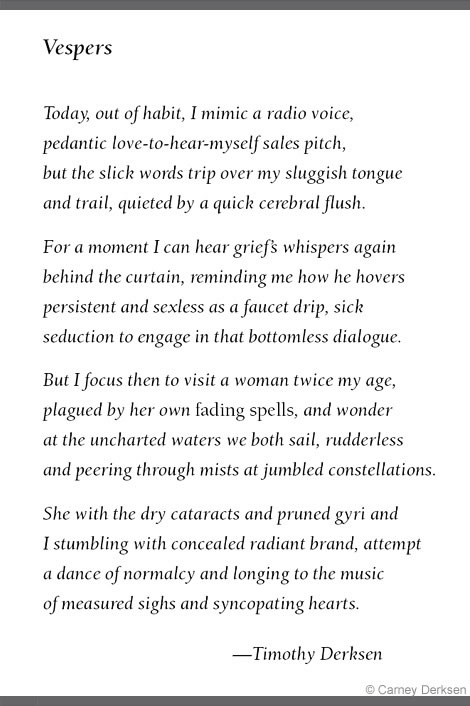
The title of the second poem (Fig. 2), Vespers, means an evening prayer, with preparation for night, sleep, or death. It encompasses reflection on the day. The first paragraph appears to describe life as it was, perhaps what was taken for granted. The “sluggish tongue” references his dysarthric problems. His embarrassment or frustration with the speech problems, “quieted by a quick cerebral flush,” appears to reflect his personal catastrophic reaction to the changes. The second paragraph embodies feelings of hidden or internal hopelessness: “I can hear grief ‘s whispers again behind the curtain.” The third paragraph references the alter ego or twinship transference.
He confronts his own damaged self and yet at the same time helps others cope with their damage or imperfections. He recognizes both his and his patient’s feelings of helplessness and narcissistic injury, with “at the uncharted waters we both sail, rudderless and peering through mists at jumbled constellations.” The last paragraph alludes to the process of transformed narcissism and self-reinvention, with a renewed ability to tolerate his imperfections. “I stumbling with concealed radiant brand, attempt a dance of normalcy.” The brand can be interpreted as a sword, symbolizing his inner strength, resiliency, and improved feelings of cohesiveness. The patient appeared to recognize the fragility of his health, perhaps even recognizing the imminence of his death: “longing to the music of measured sighs and syncopating hearts.”
The patient indicated that his practice of medicine was profoundly affected by his realization of his imperfections after surgery. His level of empathy toward his patients intensified. Given his personal experiences, he was increasingly attuned to the realities of his patients’ feelings of frustration, sadness, and despair.
Case 2
In August 1996, a 31-year-old woman experienced the onset of complex partial seizures. In September 1997, she underwent surgery for a grade 2 oligodendroglioma followed by a second surgery in February 1998. In May 1998 she was referred to the CTN for vision deficits in the right upper field, memory problems, and emotional distress.
In June 1998 neuropsychological testing indicated that she had moderate to severe deficits in complex attention, auditory processing, multi-tasking, organization, higher-level language comprehension and abstraction, and verbal learning and recall, including encoding deficits. She was experiencing significant problems with depression, anxiety, and paranoia mediated by her temporal lobe damage.
Before injury the patient had worked successfully as a mechanical engineer until May 1998. At that time she stopped work due to her health and cognitive deficits. Before her illness, she had been active in the sports of hang gliding, hiking, and running.
From July 1998 to March 1999, the patient participated in the CTN program. During that time, she experienced intermittent partial complex seizures and continued with PCV (procarbazine, lomustine, and vincristine) chemotherapy on alternating months for a 12-month period. Her medications included phenytoin, divalproex, gabapentin, sertraline hydrochloride, clonazepam, and lorazepam. During this time, she also enrolled in a local community college to study graphic arts and worked as a volunteer.
She received intensive psychotherapy during and after her participation at CTN. She was seen two to four times per month by a neuropsychologist and monthly by her psychiatrist. Treatment focused on her overall emotional status, including her depression; the manifestations of her catastrophic reactions; finding quality of life with her school and volunteer work; and realistic decision making related to her health status, including advanced directives. As part of psychotherapy, she was involved in extensive journaling, art therapy, and computer graphics. These media were highly effective for allowing her to express her feelings about her life-altering events.
The patient effectively depicted the contrast between her life before and after her illness (Fig. 3). The colors denote the freedom and happiness of her life before her illness. The airplane denotes the hang gliding she enjoyed while the headstones represent friends she had lost to this dangerous sport. As the plane hits the barbed wire, she is confronted with the end of her prediagnosis lifestyle. Instead, she sees barrenness, starkness, the gray of her depression, and the emptiness she so often experienced. Looking back, the eye may represent that she can see how things used to be; looking forward, it sees the chains that denote her feelings of being trapped by her circumstances.
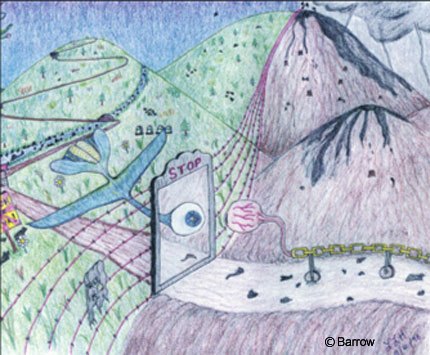
Another picture represents the roadmap of her life (Fig. 4). The green mountains represent her health and happiness. In an instant she is struck down by a lightning bolt. Her face and tears then connote feelings of darkness and desolation. The ADHNR (Adult Day Hospital Neurological Rehabilitation) bridge shows her path to recovery, allowing her to determine the course of her journey. She is faced with choices: an upward path to contentment, a difficult declining path that ends with death in the form of the dead tree. The picture shows the transformation from disorganization to organization, suggesting the self-reinvention and transformed narcissism, as she finds new paths to her existence, albeit for a shortened time.

In March 2001, the patient underwent a third surgery. By September 2001, the tumor had spread to the ventricular system. From October 2001 her neurological condition steadily declined until her death on February 1, 2002.
The CTN maintains a strong commitment to research, with emphasis on the efficacy of the intensive milieu approach to neurorehabilitation. Two studies have evaluated the level of patients’ productivity as long as 11 years after discharge from the program.[7,8] At the time of this follow-up study, about 222 patients had participated in the Work Re-Entry program. The CTN staff conducted a structured telephone survey to obtain a wide variety of information. For this study, current work/school status and job/school activity since discharge from CTN were analyzed.
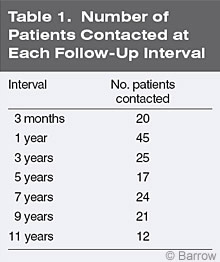
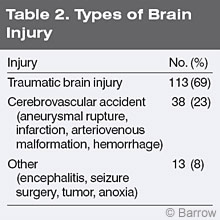
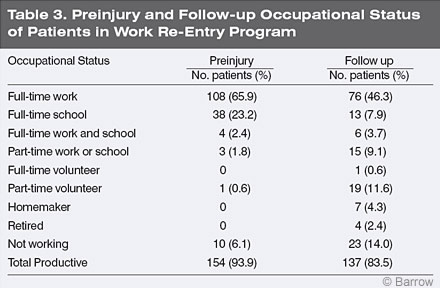
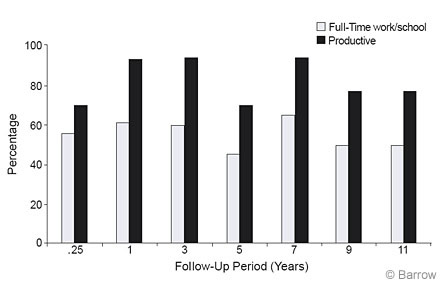
Patients who completed the Work Re-Entry program at CTN were contacted by telephone at the following intervals after discharge: 3 months, 1 year, 3 years, 5 years, 7 years, 9 years, and 11 years (Table 1).8 One hundred and sixty-four patients (66% males, 34% females) representing 74% of the total eligible CTN patients participating in the Work Re-Entry program were contacted. The mean age of patients at time of injury was 34 years (range, 14 to 64 years). The mean educational level of patients was 14 years (range, 8 to 21 years). The mean interval from their injury to their admission was 13.9 months (range, 0.6 to 318 months), and the mean length of treatment was 6 months (range 0.8 to 18 months). Most patients had a traumatic brain injury (Table 2). Before injury about 94% of the patients were productive in some capacity (Table 3), a selection criteria for participation in the CTN program.
At follow-up, 67% of the patients were involved in competitive gainful work, school, or both (Table 3).[8] Of the total sample, 84% were productive in some capacity, including volunteer work (Table 3). Based on a Chi-square analysis, there was no decline in the level of productive or full-time work/school as a function of follow-up period (Fig. 5). This finding suggested that there were enduring benefits from milieu-oriented rehabilitation.
Summary
This article represents an overview of the clinical and research endeavors at the CTN program. The extensive influence of Dr. Gustavo Lage in the psychotherapeutic process of patients with acquired brain injury was described. Case studies were included to illustrate the diverse and complex experience of loss and adaptation after brain injury. The empirical underpinnings of the milieu adds credence to the efficacy and enduring benefits of milieu-oriented neurorehabilitation.
References
- Baker HS, Baker MN: Heinz Kohut’s self psychology:An overview. Am J Psychiatry 144:1-9, 1987
- Goldstein K: The effect of brain damage on the personality. Psychiatry 15:245-260, 1952
- Jourard SM: The Transparent Self. New York: Van Nostrand Reinhold, 1971
- Klonoff PS, Lage GA: Narcissistic injury in patients with traumatic brain injury. J Head Trauma Rehabil 6:11-21, 1991
- Klonoff PS, Lage GA: Suicide in patients with traumatic brain injury: Risk and prevention. J Head Trauma Rehabil 10:16-24, 1995
- Klonoff PS, Lage GA, Chiapello DA: Varieties of the catastrophic reaction to brain injury: A self psychology perspective. Bull Menninger Clin 57:227-241, 1993
- Klonoff PS, Lamb DG, Henderson SW: Milieubased neurorehabilitation in patients with traumatic brain injury: Outcome at up to 11 years postdischarge. Arch Phys Med Rehabil 81:1535-1537, 2000
- Klonoff PS, Lamb DG, Henderson SW: Outcomes from milieu-based neurorehabilitation at up to 11 years post-discharge. Brain Inj 15:413-428, 2001
- Klonoff PS, Lamb DG, Henderson SW, et al: Milieu-based neurorehabiliation at the Adult Day Hospital for Neurological Rehabiliation, in Christensen AL, Uzell BP (eds): International Handbook of Neuropsychological Rehabilitation. New York: Plenum Publishing, 2000, pp 195-213
- Kohut H: Forms and transformations of narcissm, in Ornstein P (ed): The Search of the Self. New York: International Universities Press, 1966, pp 427-460
- Kohut H: The Analysis of the Self. New York: International Universities Press, 1971
- Kohut H: How Does Analysis Cure? Chicago: University of Chicago Press, 1984
- Kohut HS: Thoughts on narcissism and narcissistic rage. Psychoanal Study Child 2:399, 1973
- Lage GA, Nathan HK: Psychotherapy, Adolescent and Self-Psychology. New York: International Universities Press, 1991
- Marohn R: The psychology of the self. Clin Update Adol Psychiatry 1:4, 1983
- Prigatano GP, Fordyce DJ, Zeiner HK, et al: Neuropsychological Rehabilitation After Brain Injury. Baltimore: Johns Hopkins University Press, 1986
- Schwaber EA: Narcissism, self psychology and the listening perspective. Ann Psychoanal 9:115-131, 1981
- Stern D: The Interpersonal World of the Infant. New York: Basic Books, 1985
- Terman DM: Aggression and narcissistic rage: A clinical elaboration. Ann Psychoanal 3:239-255, 1975
- Winnicott DW: The Maturational Process and the Facilitating Environment. New York: International Universities Press, 1965
- Wolf ES: Treating the Self: Elements of Clinical Self Psychology. New York: Guilford, 1988