
Resolution of Status Epilepticus After Subdural Grid Recording and Multiple Subpial Transections
Ruth E. Bristol, MD
Pankaj Gore, MD
David Treiman, MD*
Kris A. Smith, MD
Divisions of Neurological Surgery and *Neurology, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
Status epilepticus remains a potentially fatal consequence of poorly controlled seizures. Medically intractable status epilepticus poses a management challenge for neurological and neurosurgical teams. We present a case in which subdural grid electrodes were used to record cortical discharges and to guide the subpial transections. A 29-year-old woman in status epilepticus was refractory to all medical therapy, including barbiturate coma. As an alternative to withdrawal of care, the patient’s family elected to proceed with subdural grid mapping after surface electrodes vaguely localized the seizure focus to the left hemisphere. Multiple subpial transections were subsequently performed, and the status epilepticus resolved. The patient remains on three oral antiepileptic drugs, and no seizures have been recorded on electroencephalography. After undergoing 6 weeks of inpatient neurorehabilitation, she returned home with her family and is seeking employment. This case illustrates a potentially life-saving technique for the treatment of refractory status epilepticus. Multiple subpial transections should be considered for patients with medically intractable status epilepticus without an obvious etiology. When localization with surface electrodes is poor, especially in eloquent cortex, subdural grid recording can be used to direct the transections to minimize neurological deficits.
Key Words: epilepsy, intracortical connections, multiple subpial transections, status epilepticus.
Abbreviations Used: CT, computed tomography; EEG, electroencephalography; MR, magnetic resonance
In terms of the duration of seizure activity, the definition of status epilepticus has recently been questioned.[6] It has been proposed that any one seizure or multiple seizures without full recovery of consciousness lasting more than 5 minutes should be classified as status. Regardless of the strict definition of the disorder, this article addresses a treatment option for patients whose status epilepticus has become refractory to medical treatment.
Multiple subpial transections are performed by making horizontal cuts in the cortex at 3- to 5-mm intervals to interrupt the epileptogenic spread along horizontal fibers; vertically oriented functional fibers are spared. The technique takes advantage of the columnar organization of the cerebral cortex while disrupting the lateral communication of epileptogenic discharges.[8]
Case Report
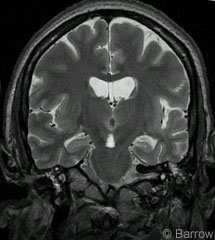
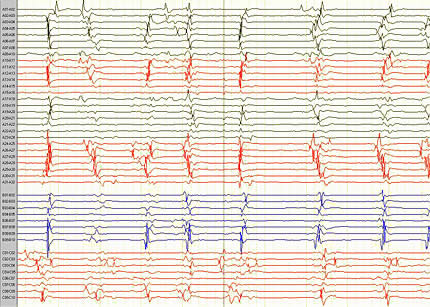
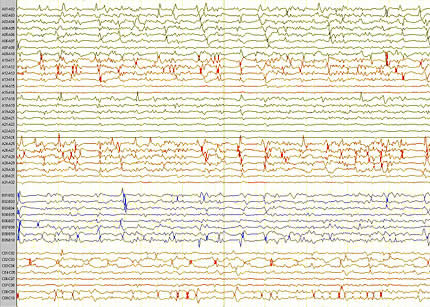
At admission a 29-year-old woman was comatose, in status epilepticus. She had a history of poorly controlled seizures, but MR images showed no focal abnormality (Fig. 1). Seizure activity was refractory to phenytoin, valproic acid, phenobarbital, gabapentin, and levetiracetam. Three days after admission, the patient was placed in a pentobarbital coma and her seizures resolved. Six days later an attempt was made to wean the patient from barbiturates, but seizure activity recurred. Barbiturates were restarted, but the status epilepticus remained refractory. During the initial 15 days of her admission, surface electrodes localized the origin of the seizure spikes to the left hemisphere (Fig. 2).
Because her seizures were refractory and located in the left hemisphere, her poor prognosis and the prospect of withdrawing care were discussed with the family. Surgical intervention for placement of subdural grids with subsequent lobectomy, hemispherectomy, or subpial transections, with their low expected success rates, were offered as treatment options. The decision was made to place the subdural grid and likely to proceed with a temporal lobectomy depending on the results of the grid placement.
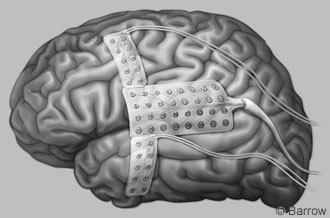
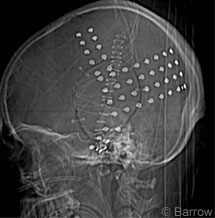
On Day 17 of her admission, a craniotomy, extending over the inferior, middle, and superior temporal gyri and across the central sulcus and supplementary and primary motor areas, was performed to place the subdural grid (Figs. 3 and 4). Contrary to our preoperative suspicion, two days of mapping showed the phase reversals to be centered around the Rolandic fissure. The patient then underwent multiple subpial transections in the angular gyrus, superior temporal gyrus, and suprasylvian frontal lobe (Figs. 5 and 6).
Subsequently, the patient was weaned from barbiturates. Four days later she resumed following commands. During this period she had a persistent twitch of her left chin, but it did not correlate with seizure activity on EEG (Fig. 7). Six weeks after surgery, she had no focal weakness. She was able to dress with minimal assistance and to ambulate 150 feet. Her tracheostomy and feeding tubes were removed during her neurorehabilitation stay. She is now fully communicative without aphasia and seeking employment while living at home. The facial twitching persists, although EEG has indicated no current seizure activity. She remains on levetiracetam, lorazepam, and phenytoin.
Discussion
The incidence of status epilepticus is estimated to range between 60,000 to 150,000 patients per year.[2] Most cases occur in the pediatric population. Of patients presenting with status epilepticus, almost 50% are newly diagnosed with epilepsy. Febrile seizures and infections of the nervous system are common predisposing factors in children, whereas cerebrovascular accidents are the most common cause in the elderly. An underlying structural lesion is more common in adults than in children. The mortality rate associated with status epilepticus is estimated at 10 to 12%. Death, however, is more likely to result from the underlying cause of the status epilepticus than from the complications of status epilepticus itself. Irreversible changes occur in neurons after 20 minutes of seizure activity, and cell death begins after 60 minutes.[4] The best outcomes without neurological injury are achieved when seizure activity is resolved, pentobarbital coma is begun within an hour of the onset of status epilepticus, or both. Cardiac, respiratory, renal, and other metabolic systems are also stressed.
Status epilepticus that initially fails to respond to lorazepam or diazepam and subsequently fails to respond to second-line therapies such as phenytoin is defined as refractory.[5] Pharmacotherapy remains the first-line treatment for status, but patients with refractory status epilepticus and no underlying structural abnormality are a management challenge. Even when seizure activity can be controlled temporarily with medication, some patients experience recurrent status epilepticus with changes in medication or dose reductions. A randomized controlled trial comparing lorazepam alone, phenytoin alone, diazepam and phenytoin together, and phenobarbital found that these agents were equally effective.[9]
For patients who continue to have status epilepticus despite receiving multiple medications, including barbiturate anesthesia, surgical intervention is the final option. Resection of seizure foci and hemispherectomy are options for focal abnormalities or for patients with a damaged hemisphere with less functional significance. However, callosal sectioning and multiple subpial transections should be considered for patients without a discrete underlying lesion, especially when discharges localize to eloquent cortex.

Surface electrodes are useful in localizing seizure foci in many patients, but intracranial depth electrodes and implantable grids provide more definitive localization.[1] When multiple subpial transections are performed, the increased specificity for localization greatly decreases the risk to eloquent cortex. Intraoperative electrocorticography can also be used to guide resection, although the amount of tissue that needs to be removed may be overestimated.[3] Furthermore, the use of electrocorticography is limited in patients acutely suffering from status epilepticus. We favor the use of subdural grids for the ability to record for an extended period. Rather than restricting the recording session to the length of surgery, grids can be left in place while medications are adjusted and patients undergo provocative testing. Grid mapping also helps identify eloquent motor regions that can be preserved.
The persistence of facial twitching in our patient is a concern. Several EEG studies have failed to correlate her facial movements and electrical discharges, but they persist despite changes in medication. A 6-year-old patient who also underwent subpial transections after 62 days of status epilepticus likewise had persistent facial twitching.[1] In neither case were the twitches accompanied by an alteration in consciousness, and the patients appear to be only minimally bothered by them.
Several authors have discussed factors that determine the timing of surgical intervention for status epilepticus.[1,7] Prolonged medical management is associated with other complications, such as hypotension, myocardial and respiratory depression, and increased risks of infection and poikilothermia. Delaying surgery may be an option for patients whose status epilepticus is controlled with medication. However, we believe that surgical intervention should be considered early in the course of refractory status epilepticus. In our patient, the issue of withdrawing care had been raised—the family turned to surgical intervention as a final, potentially life-saving option.
References
- Cascino GD, Boon PAJM, Fish DR: Surgically remediable lesional syndromes, in Engel J, Jr. (ed): Surgical Treatment of the Epilepsies. Second Edition. New York: Raven Press Ltd., 1993, pp 77-86
- D’Giano CH, Del CG, Pomata H, et al: Treatment of refractory partial status epilepticus with multiple subpial transection: Case report. Seizure 10:382-385, 2001
- Engel J, Jr: Approaches to the localization of the epileptogenic lesion, in Engel J, Jr. (ed): Surgical Treatment of the Epilepsies. New York: Raven Press, 1987, pp 75-100
- Fountain NB, Lothman EW: Pathophysiology of status epilepticus. J Clin Neurophysiol 12:326-342, 1995
- Golf M, Paice JA, Feulner E, et al: Refractory status epilepticus. J Palliat Med 7:85-88, 2004
- Lowenstein DH, Bleck T, Macdonald RL: It’s time to revise the definition of status epilepticus. Epilepsia 40:120-122, 1999
- Ma X, Liporace J, O’Connor MJ, et al: Neurosurgical treatment of medically intractable status epilepticus. Epilepsy Res 46:33-38, 2001
- Morrell F, Whisler WW, Bleck TP: Multiple subpial transection: A new approach to the surgical treatment of focal epilepsy. J Neurosurg 70:231-239, 1989
- Treiman DM, Meyers PD, Walton NY, et al: A comparison of four treatments for generalized convulsive status epilepticus. Veterans Affairs Status Epilepticus Cooperative Study Group. N Engl J Med 339:792-798, 1998