
Hemangioblastoma with a “Dural Tail” Sign: Case Report
Paul Detwiler, MS, MD
Randall W. Porter, MD
Elad I. Levy, BS*
Robert F. Spetzler, MD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
*Current address: University of Pittsburgh, Pittsburgh, PA
Abstract: A 41-year-old female with persistent headaches, dizziness, and visual scotomas underwent magnetic resonance (MR) imaging, which demonstrated a mass in the right cerebellopontine angle with a “dural tail” sign. Based on the radiographic appearance of the lesion, meningioma was the preliminary diagnosis. However, surgical resection revealed the tumor to be a hemangioblastoma. To the best of our knowledge, this is the first reported case of a hemangioblastoma demonstrating the “dural tail” sign on MR imaging.
Key Words: dural enhancement, dural tail sign, hemangioblastoma, magnetic resonance imaging, meningioma
The “dural tail” sign was originally proposed as a highly specific finding associated with meningiomas on magnetic resonance (MR) imaging studies.(1) This finding has now been described in association with acoustic neuromas, metastases, lymphomas, chordomas, sarcoidoses, adenoid cystic carcinomas, and pituitary adenomas but not with hemangioblastomas.(3-5,7,8)
Case Report
A previously healthy 41-year-old female sought treatment after experiencing dizziness, imbalance, incoordination, severe occipital headaches, and visual scotomas for 4 months. Physical examination showed mild bilateral hyperreflexia, dysmetria, and dizziness.
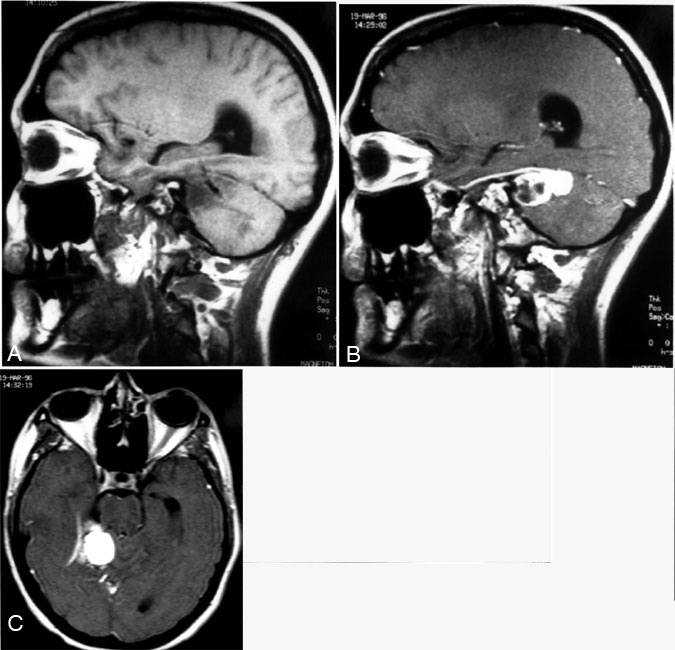
MR imaging (Fig. 1) revealed a contrast-enhancing extraaxial mass (2.2 x 3.8 x 3.2 cm) in the right cerebellopontine angle compressing the cerebellar hemisphere. Surrounding edema was present. On contrast-enhanced images, the mass had a broad-based dural attachment to the inferior right tentorial leaf with a “dural tail” sign. Accordingly, the presumptive diagnosis of meningioma was made.
The patient underwent a stereotactic wand-guided (ISG, Mississauga, Ontario, Canada) right retrosigmoid craniotomy. A large feeding branch from the superior cerebellar artery and draining veins were present where the tumor abutted the dura; however, the tumor was not dural based. Furthermore, the lesion was red. Based on these findings, the lesion was thought to be a hemangioblastoma.
The operative approach was adjusted accordingly. The borders of the tumor were separated carefully, and a temporary aneurysm clip was placed on the feeding artery. After the clip was placed, the tumor softened and darkened, allowing its circumferential dissection and removal in one piece.
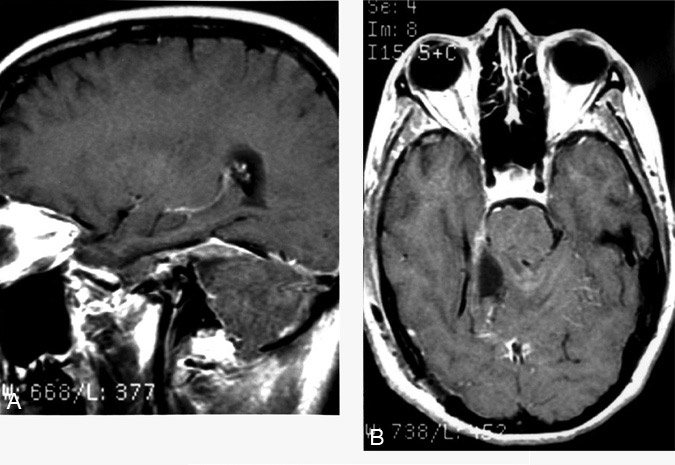
Histopathologic evaluation of the tumor revealed a typical hemangioblastoma with characteristic interstitial foam cells separated by thin-walled vascular channels. Immediate postoperative MR imaging showed no evidence of residual tumor or the “dural tail” sign (Fig. 2). The patient’s preoperative symptoms resolved, and she was neurologically intact on follow-up examination.
Discussion
The appearance of thickened, enhancing dura adjacent to and tapering away from a dural-based meningioma on MR imaging was first described by Wilms and colleagues in 1989.10 In 1990, Goldsher et al.1 coined the term “dural tail” to describe the dural enhancement of some meningiomas on MR imaging. They proposed a rigid definition with three criteria for the identification of dural tails. First, the dural enhancement must be present on at least two consecutive sections through the tumor and in more than one imaging plane. Second, its thickness must be greatest adjacent to the tumor and then taper away from it. Finally, on T1-weighted MR imaging the adjacent dura must have a higher signal intensity than the tumor.1
Early reports suggested that the “dural tail” sign was associated with approximately two-thirds of all meningiomas, for which it was believed to be highly specific.1,6 Several theories were proposed to account for this enhancement: extension of the tumor into the dura mater,10proliferation of fibrous and loose connective tissue,9 or invasion of meningothelial nodules. Enhancing cortical veins mimicking the “dural tail” sign have also been described.6
Other tumors, including acoustic neuromas, metastases, lymphomas, chordomas, neurosarcoidoses, adenoid cystic carcinomas, and pituitary macroadenomas, also exhibit the “dural tail” sign.3-5,7,8 However, a “dural tail” sign has not yet been reported in association with a hemangioblastoma. In our patient, the “dural tail” sign did not adhere rigidly to the original definition proposed by Goldsher et al.1 and was likely the result of a vascular structure mimicking a “dural tail.” This phenomenon has been described by Nägele and coworkers.6 On T1-weighted MR imaging, the typical appearance of a hemangioblastoma is a contrast-enhancing nodule surrounded by a low-intensity signal. Arteries and veins may appear as serpiginous signal voids.2
Conclusions
The literature indicates that most tumors with a “dural tail” sign are meningiomas. The risk of significant bleeding during the resection of a hemangioblastoma, however, should prompt its consideration in the differential diagnosis.
References
1. Goldsher D, Litt AW, Pinto RS, et al: Dural “tail” associated with meningiomas on Gd-DTPA-enhanced MR images: Characteristics, differential diagnostic value, and possible implications for treatment. Radiology 176:447-450, 1990
2. Hasso AN, Bell SA, Tadmor R: Intracranial vascular tumors. Neuroimaging Clin N Am 4:849-870, 1994
3. Koenigsberg RA, Patil K: Pituitary apoplexy associated with dural (tail) enhancement (letter). AJR 163:227, 1994
4. Kutcher TJ, Brown DC, Maurer PK, et al: Case report. Dural tail adjacent to acoustic neuroma: MR features. J Comput Assist Tomogr 15:669-670, 1991
5. Morioka T, Matsushima T, Ikezaki K, et al: Intracranial adenoid cystic carcinoma mimicking meningioma: Report of two cases.Neuroradiology 35:462-465, 1993
6. Nägele T, Petersen D, Klose U, et al: The “dural tail” adjacent to meningiomas studied by dynamic contrast-enhanced MRI: A comparison with histopathology. Neuroradiology 36:303-307, 1994
7. Senegor M: Prominent meningeal “tail sign” in a patient with a metastastic tumor. Neurosurgery 29:294-296, 1991
8. Tien RD, Yang PJ, Chu PK: “Dural tail sign”: A specific MR sign for meningioma? J Comput Assist Tomogr 15:64-66, 1991
9. Tokumaru A, O’uchi T, Eguchi T, et al: Prominent meningeal enhancement adjacent to meningioma on Gd-DTPA-enhanced MR images: Histopathologic correlation. Radiology 175:431-433, 1990
10. Wilms G, Lammens M, Marchal G, et al: Thickening of dura surrounding meningiomas: MR features. J Comput Assist Tomogr 13:763-768, 1989