
Normal Pressure Hydrocephalus (NPH)
At a Glance
- Normal pressure hydrocephalus (NPH) is a condition where cerebrospinal fluid accumulates in the brain’s ventricles, causing them to enlarge, despite normal pressure readings.
- Classic symptoms include gait disturbance (shuffling walk), urinary incontinence, and cognitive decline.
- Diagnosis is based on clinical presentation, an MRI of the brain, and often confirmed with a high-volume lumbar puncture or extended cerebrospinal fluid (CSF) drainage test.
- Treatment typically involves surgical placement of a shunt to drain excess fluid, often resulting in significant improvement.
Overview
Normal pressure hydrocephalus (NPH) describes an abnormal buildup of cerebrospinal fluid (CSF) in the hollow cavities of the brain called cerebral ventricles.
A clear fluid cushioning the brain and spinal cord, CSF provides nutrients, removes waste, and helps maintain intracranial pressure. Usually, just enough CSF is made each day and absorbed by the body, but in NPH, the balance between CSF production and absorption is disrupted. This causes CSF to build up in the ventricles, which in turn causes them to enlarge.
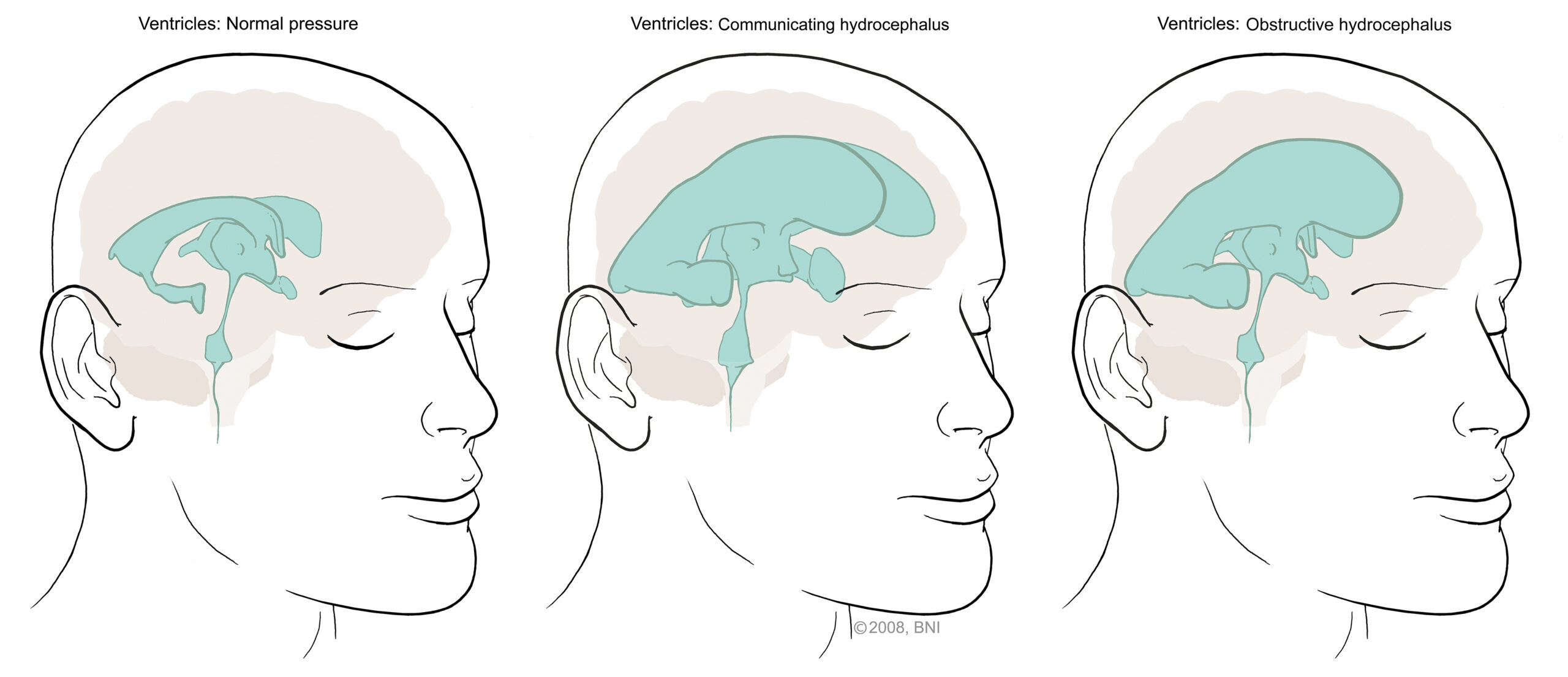
Because the ventricles enlarge to accommodate the extra fluid, intracranial pressure is generally within normal limits—hence the name “normal pressure” hydrocephalus.
There are two types of NPH:
- Idiopathic NPH: In idiopathic NPH, there is no identifiable cause. It’s thought to develop from gradual, age-related changes in the ability to absorb CSF or from subtle, gradual damage to CSF pathways.
- Secondary NPH: This form of NPH stems from a known cause that affects CSF reabsorption, such as a traumatic brain injury (TBI), brain surgery, brain tumor, subarachnoid hemorrhage, or a brain infection like meningitis.
Generally, adults have about five fluid ounces of CSF in their bodies at any given time—less than a small glass of water. To keep that amount of CSF constant, the body continuously creates, circulates, and reabsorbs the fluid. But when your body cannot properly circulate or reabsorb the CSF, too much fluid builds within the skull and compresses the brain. This is what causes symptoms of NPH and can permanently damage or destroy brain tissue if left untreated.
Since NPH primarily affects older adults, it can be particularly challenging to diagnose. This is because its symptoms tend to mimic other neurodegenerative disorders, like Alzheimer’s disease and Parkinson’s disease.
What causes normal pressure hydrocephalus (NPH)?
While it’s not entirely understood, a common theory is that NPH is caused by the dysfunction of arachnoid granulations, which are responsible for reabsorbing CSF into the bloodstream. When these arachnoid granulations are damaged, overall cerebrospinal fluid (CSF) absorption decreases.
- Idiopathic NPH: Idiopathic NPH, which accounts for roughly 50%of NPH cases, is thought to be caused by one or more age-related issues with how the body makes, circulates, and reabsorbs CSF.
- Secondary NPH: Secondary NPH is caused by another medical condition—a brain aneurysm, brain hemorrhage, brain tumor, stroke, brain infection, or traumatic brain injury—that affects how your body makes, circulates, or reabsorbs CSF.
There’s also evidence that NPH may have a connection to degenerative brain conditions. In fact, 30% or more of people diagnosed with NPH may also have coexisting neurodegenerative conditions, like Alzheimer’s disease or Parkinson’s disease.

Normal Pressure Hydrocephalus (NPH) Symptoms
Normal pressure hydrocephalus (NPH) symptoms most closely resemble the symptoms of dementia, as they start gradually and typically worsen over a matter of months. Different from dementia, however, are the condition’s hallmark symptoms, known as Hakim’s triad, named after Salomon Hakim, MD, PhD, who first defined NPH more than 50 years ago.
A combination of these three symptoms is considered the defining characteristic:
- Changes to the way you walk: Known as gait disturbance, this symptom is often the first to appear and can be the most prominent symptom. This can look like shorter and more unsteady steps taken in a “shuffling” manner, or having trouble lifting your feet—some report feeling as though there’s a magnetic force holding their feet to the ground. It may also look like walking uncertainly or freezing, as though you can’t quite figure out how to take a step after starting to walk.
- Cognitive impairment: This can look like slowed thinking, forgetfulness, confusion, concentration or memory problems, or difficulty paying attention. It can also present as struggling to manage your thoughts, emotions, or actions, or losing interest in things you used to enjoy.
- Urinary incontinence: This symptom tends to start as urinary urgency—feeling as though you need to urinate often or have an extreme need to relieve yourself—then progresses to incontinence, or completely losing control of your bladder. Unlike difficulty walking or cognitive impairments, this symptom tends to occur later in the course of NPH.
Researchers estimate that between 50% and 75% of people with NPH will have all three of these symptoms at the same time. That said, these symptoms alone don’t mean you have NPH. An accurate diagnosis requires a thorough evaluation by a healthcare professional.
Normal Pressure Hydrocephalus (NPH) Diagnosis
It’s not uncommon for the diagnosis of NPH to come late, due to the slow progression of subtle and ill-defined symptoms that are often initially attributed to aging. Doctors frequently misdiagnose individuals with NPH as having Parkinson’s or Alzheimer’s first, and, to further complicate diagnosis, nearly 30% of people with NPH also have Alzheimer’s or a similar neurodegenerative disease.
If you have symptoms of NPH, your doctor will perform the following diagnostic tests:
- Physical and neurological exam: When NPH is suspected, it’s recommended that a neurologist with extensive experience assessing brain disorders be involved. First, they will ask about your symptoms, overall health, and family history. Next, they’ll complete an examination to assess your neurological function, including cognitive function, reflexes, coordination, strength, and sensation. An evaluation of how you or your loved one walks will also likely be performed.
- Brain imaging: Brain imaging is crucial in diagnosing NPH, as magnetic resonance imaging (MRI) or a computed tomography (CT) scan will help pinpoint enlarged ventricles. While an MRI provides highly detailed images of the brain, including ventricles and tissue, CT scans rely on X-rays to create detailed cross-sectional images of the brain. They can be used when an MRI is not recommended.
- Testing of cerebrospinal fluid (CSF): This diagnostic tool involves a lumbar puncture, where a needle is inserted into the lower part of your spinal canal to collect CSF. Your doctor will measure the pressure of your CSF as you lie on your side, which will help distinguish it from other forms of hydrocephalus.
- Physical Therapy assessment: Physical therapy will evaluate your walking before and after the lumbar puncture to assess if removing CSF temporarily improves the symptoms of walking difficulty, cognitive impairment, and urinary incontinence.
Your healthcare provider may also recommend other tests to help rule out other conditions.
Overall, NPH continues to be challenging to diagnose because of its symptom overlap with dementia-based diseases. However, NPH is one of the few causes of dementia-like symptoms that can be controlled or even reversed with treatment.

Normal Pressure Hydrocephalus (NPH) Treatment
Unlike dementia or Alzheimer’s, normal pressure hydrocephalus (NPH) can potentially be reversed through treatment. The best odds for reversing NPH are when doctors diagnose the condition early—the greater the delay in diagnosis and treatment, the more likely it is to cause permanent or severe damage to your brain from prolonged high CSF pressure.
The most common and effective treatment for idiopathic NPH is ventriculoperitoneal (VP) shunt surgery. A VP shunt consists of three parts:
- Ventricular catheter: This part is inserted into a lateral ventricle in the brain to collect excess cerebrospinal fluid (CSF).
- Valve mechanism: This piece controls the rate and pressure of CSF drainage and can be pre-set or programmed externally via a magnet.
- Distal catheter: This part runs under the skin from the head, down the neck, and into the abdomen, where the CSF is absorbed.

During this procedure, a neurosurgeon inserts the shunt into a ventricle in the brain via a small incision in your scalp and a hole drilled into your skull. The valve mechanism is connected and passed under your skin from your head, neck, and chest to your abdomen. The extra fluid in your brain will then flow through the shunt into your abdomen, where your body reabsorbs it, and the ventricles in your brain return to their normal size.
Shunting for NPH tends to relieve symptoms quickly—you may notice the most dramatic improvement in gait or walking ability. Cognitive and urinary symptoms may also improve, but those can occur less predictably. That said, most people will show improvements within hours or days. However, after surgery, a full recuperation period is necessary to recover. The shunt will likely stay in place for the rest of your life.
Since secondary NPH stems from another primary condition, healthcare professionals can cure or reverse it only by treating the primary condition. This means that the treatment for secondary NPH encompasses a spectrum of treatments, such as brain surgery, tumor removal, endovascular surgery, and more.
Currently, there are no known effective nonsurgical treatments for NPH. Medications that remove excess fluid from the body, such as diuretics, haven’t shown the ability to relieve symptoms.
Common Questions
How common is normal pressure hydrocephalus?
Normal pressure hydrocephalus (NPH) is considered uncommon, but it’s likely underdiagnosed in older adults. Statistics show that approximately 0.2%of people between the ages of 70 and 80 have the condition, while around 5% of people over 80 do. However, according to the Hydrocephalus Association, a study has estimated that more than 80%of NPH cases remain unrecognized or untreated.
Despite being relatively rare, NPH is a treatable cause of dementia-like symptoms, so recognizing it is essential.
Who gets normal pressure hydrocephalus?
Normal pressure hydrocephalus (NPH) is most often diagnosed in people between the ages of 60 and 80, although the rates of incidence increase after 65. It’s very rare in younger adults unless there’s a clear secondary cause, like a traumatic brain injury (TBI), brain surgery, or infection. NPH affects men and women equally.
While age is the most significant risk factor for NPH, a history of brain trauma, hemorrhage, infection, or surgery increases the risk of secondary NPH. There may also be genetic or vascular (blood vessel) components, but these are poorly understood.
What is the difference between normal pressure hydrocephalus and hydrocephalus?
The key difference between normal pressure hydrocephalus (NPH) and traditional hydrocephalus is the mechanism of the pressure from the cerebrospinal fluid (CSF).
Even though both conditions involve the buildup of CSF, in hydrocephalus, the CSF builds up rapidly, causing escalating symptoms due to the increasing pressure. In NPH, the pressure inside your skull isn’t unusually or dangerously high—hence the term “normal pressure”—and symptoms gradually intensify.
What is the prognosis for someone with normal pressure hydrocephalus?
A favorable prognosis is more likely when normal pressure hydrocephalus (NPH) is diagnosed early, when walking or incontinence challenges are experienced before cognitive symptoms, and when symptoms improve after a lumbar puncture that removes cerebrospinal fluid (CSF). The prognosis also tends to be favorable when you or your loved one has secondary NPH that doctors can reverse with treatment.
A less favorable outcome can occur when there is a delay in diagnosis or treatment, cognitive symptoms develop early or worsen quickly, or you have another degenerative brain condition, such as Alzheimer’s disease. When untreated, NPH can lead to permanent disability.
Can normal pressure hydrocephalus be prevented?
Unfortunately, idiopathic normal pressure hydrocephalus (NPH) cannot be prevented, since its exact cause remains unknown and it often occurs without an apparent trigger. This means there’s no established strategy to stop it from developing.
However, secondary NPH that occurs after a brain injury or an infection can be considered partially preventable by reducing your risk factors for these underlying causes.
- Prevent head trauma: Remember to use seatbelts, helmets, and appropriate fall prevention strategies, especially if you’re above age 65.
- Manage vascular risk factors: Conditions like high blood pressure, diabetes, and atherosclerosis can contribute to microvascular damage in your brain, disrupting the flow of CSF.
- Manage any postoperative complications: After a neurosurgical procedure, ensure you have a robust care team to provide thorough monitoring.
- Prevent and properly manage brain infections: Seek out early treatment of infections that can damage your central nervous system, like meningitis.


