
The History of Neuroscience Nursing: A Barrow Perspective
Author
Virginia Prendergast, RN, NP-C, CNRN
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
The development of neuroscience nursing at the Barrow Neurological Institute parallels both the development of the institution itself and the specialization of neuroscience nursing. During the past 40 years, Barrow nurses have established themselves as leaders within the institution and within the nursing profession. This article describes the emergence of neuroscience nursing on a national level and specifically chronicles its progress as a nursing specialty at Barrow.
Key Words: history, neuroscience, nursing
Neuroscience nursing was first reported as an observational practice under the tutelage of Sir Victor Horsley, a neurosurgeon at the world’s first neurological institute, the National Hospital in Queen’s Square, London. In the 1870s, Sir Horsley invited nurses to observe surgery to enable them to better care for the patients postoperatively. During this same period, J.M. Charcot, MD, a neurologist at Salpêtrière in France and a recognized teacher, writer, and mentor, encouraged nurses to learn about the central nervous system.[6]
Although women have always been considered caretakers of the sick and injured, they were rarely trained to provide specialized care.[5] During the Crimean War in the mid1850s, Florence Nightingale established the first standardized training for nurses. Neuroscience nursing began to emerge as a specialty in response to advances in the fields of neurosurgery and neurology as well as in response to the need to care for individuals injured during World Wars I and II and the Korean War.
During the Vietnam War, Margarethe Cammermeyer, RN, served as the head nurse in the neurosurgical unit in the 24th Evacuation Hospital during the Tet Offensive in 1968.[2] Heavy casualties were sustained during this battle, and Cammermeyer was faced with caring for patients with devastating head injuries. Despite limited resources, limited staff, and the overwhelming need to care for an increasing number of critically ill patients, Cammermeyer remained committed to providing care, the human touch, and a sense of compassion to patients. No neurosurgical patient was allowed to be removed from life support unless she was at the bedside so that “no one would die alone” (Cammermeyer M, personal communication, 1995). The simultaneous provision of expert nursing care combined with a sense of compassion began to lay the foundation for neuroscience nursing care as it is known today. This article traces the growth in the profession of neuroscience nursing as it developed at Barrow Neurological Institute and within the greater context of neuroscience nursing.
Clinical Practice
The 1960s and 1970s
At Barrow, neuroscience nursing officially began on the day that the first units opened in 1962. In the beginning, being a nurse at Barrow translated into being a nurse in one of three newly established units: the operating room (OR), the neurosurgical intensive care unit (NICU), or the general neurosurgical-neurological ward. The combined nursing staff for the three units was 28 nurses.
Dedicated neuroscience units represented a relatively new concept to both St. Joseph’s Hospital and the nursing profession at large. While Dr. W. E. Dandy is credited with opening a three-bed specialized care unit for postoperative neurosurgical patients in 1923 at the Johns Hopkins Hospital,[7] the concept of such dedicated units was not widespread, nor did the concept of intensive care units (ICUs) take root for decades. ICUs were just beginning to appear in the late 1960s and early 1970s and typically were designated as postanesthesia care or coronary care units. In the nursing literature, a dedicated neuroscience ICU was first mentioned in 1975.[1] At the time Barrow was founded, there were no dedicated neuroscience units in Arizona.
Consistent with the national trend, the first ICU at St. Joseph’s Hospital was the coronary care unit; the second ICU was the NICU. That first NICU housed a total of 6 beds. Four beds were clustered in a general ward setting, and there were two private rooms and one hyperbaric chamber. Despite the neurosurgical title of the NICU, nurses working there treated patients with disease processes other than those with a neurological dysfunction. The NICU included patients undergoing hyperbaric oxygen therapy and renal dialysis, patients requiring support by an iron lung, and burn patients. Ultimately, these services remained a part of the care provided at St. Joseph’s Hospital, except for patients with burns. The latter were automatically transferred to Maricopa County Hospital when the burn unit opened there in the 1970s.
During these early years, scant assistive technology was available. Consequently, nursing care relied on close observation of patients and changes in their level of consciousness (LOC). As nurses and neurosurgeons recollect, the calls made to physicians from the ICU nurses were in response to changes in a patient’s LOC. When reports of a decreased LOC were communicated to the physician, nurses were instructed to give patients a “pinch of mannitol.” The LOC was the single most important assessment parameter. The NICU had no cardiac monitors. There was no invasive blood pressure monitoring. Temperatures were measured with mercury-filled thermometers, and blood pressure was measured with traditional sphygmomanometers. The only invasive lines were urinary catheters and nasogastric tubes.
In 1962, one registered nurse (RN) cared for one or two patients in the NICU. However, the staffing pattern was different on the general neurological-neurosurgical floor. Because specialized neurological units were new, it was difficult to establish staffing patterns and appropriate patient-to-nursing care ratios on the floor. At the time, the popular nursing model for patient care was referred to as Team Nursing. The Team consisted of an RN, a licensed practical nurse (LPN), and one nurse’s aide to provide nursing care for 5 or 6 patients. The RNs were responsible for performing patient assessments, reviewing laboratory results, noting orders, and all communications with physicians. The LPNs administered all medications to the patients cared for by the team. The nurses’ aide or orderly helped with the manual demands of patient care such as lifting, turning, and getting patients out of bed.
The physical component of neuroscience nursing was demanding. There were no specialized chairs to facilitate getting patients up or specially constructed slide boards to move patients from one horizontal surface to another. There were no special rinse free soaps for use during bathing. There were no electric beds. Hand cranks were used to raise or lower the head or knee position. The work was demanding, but as a former nurse who worked on the general neurosurgical ward for 20 years quipped “Of course it wasn’t easy; if it was, any nurse could do it.” The nurses who elected to work at Barrow and the physicians with whom they worked were committed to the ideal that every patient deserved a nurse who specialized in the care of the neurologically impaired.
In the early days of neurosurgery at Barrow, the array of technical items now familiar in neurosurgical ORs–surgical microscopes, the variety of aneurysm clips, and spinal instrumentation–was nonexistent. In fact, the only instrumentation available for spinal surgery was Harrington rods. During long cases, nurses recall fashioning a neurosurgical workstation by providing a swivel stool on wheels and draping two Mayo stands for the physician to rest his arms.
By the mid 1960s the patient population at Barrow was too large to be housed in the existing two units, and additional construction was begun. The sixth, seventh, and eighth floors were added in 1968. This expansion almost doubled the available bed space for neurological patients, increasing the number of beds from 37 to 74. The ICU was moved to the newly completed seventh floor in Barrow where electrocardiographic (EKG) monitors were first introduced to the NICU. Initially, there were three monitors for 10 beds. EKGs were monitored at the nurse’s discretion. In the NICU, as elsewhere around the country, it was common practice for EKG monitoring to be optional because the focus of assessment was the patient’s LOC.[1]
Barrow nurses worked an 8-hour day, evening, or night shift. On the floor, there was one head nurse for the day and evening shifts. Both the NICU and the neurosurgical OR had one head nurse. On all units the night shifts were covered by a charge nurse, who served as a resource for nursing staff and as the contact person for physicians and residents. Changes in shift were marked by the head or charge nurses conducting walking rounds from bedside to bedside, always wearing a white dress, complete with nursing cap. In the early days at Barrow, all nurses were required to wear a nursing uniform dress and cap to exhibit their professionalism (Fig. 1). However, wearing a dress was challenging when providing care to bedridden patients.
The length of hospitalization varied, depending on a patient’s diagnosis, hospital course, and family support. Patients undergoing elective surgery were admitted the day before surgery for preoperative testing and remained in the hospital 7 to 10 days after surgery. For patients admitted with a neurological diagnosis such as multiple sclerosis, the evaluation and length of stay could be 14 to 21 days.

Head-injured patients were cared for expectantly. In the 1960s, intracranial monitoring was not yet available. Increases in intracranial pressure were determined by changes in the patient’s LOC or by radiological tests such as ventriculography, during which oxygen or air was injected directly into the lateral ventricle via a twist drill penetration of the skull. Ventricular size, shape, and placement were then assessed to confirm increased intracranial pressure. Alternatively, pneumoencephalography, during which air was injected via a lumbar puncture and allowed to rise displacing cerebrospinal fluid in ventricles, was used to detect changes in intracranial mass effect associated with tumors or hydrocephalus. By the 1970s, the hospital had purchased a computed tomography (CT) scanner that could image intracranial structures. However, if pathology was suspected in the posterior fossa, the patient still underwent pneumoencephalography or ventriculography because the extensive bone in the posterior fossa almost obliterated any images seen on CT. Patients who had suffered a complete spinal injury could be hospitalized 3 to 6 months because no rehabilitation units were designated for patients with spinal cord injuries. Consequently, early Barrow nurses provided all phases of care for patients with a neurological injury or disorder. The demand of caring for these patients was great. In 1978 the Arizona Emergency Medical Systems designated St. Joseph’s Hospital as the only Level I Trauma Center for head and spine injuries in the state.
Considerable work was also involved with maintaining supplies for patient care. Bandages used for head dressings were washed after use and rewrapped on drying boards for use on the next patient. Soapsud enemas, the only type available, were made by the staff using bars of soap and bottles of water. Intravenous sites were difficult to maintain because nurses were only allowed to insert butterfly needles, which rarely lasted more than a day.
Overall, the early technology could be described as straightforward. Tracheostomy cannulas were available only in one type–metal. All nasogastric tubes were initially used for gastric decompression. Later the same tube was used for bolus enteral tube feedings. Pulse oximetry monitors did not exist.
As the number of patients at Barrow grew, so did the demands placed on the nurses who cared for them. In the 1970s, St. Joseph’s Hospital hired a clinical nurse specialist (CNS). A CNS is a master’s prepared RN who helps educate nursing staff and patients, acts as a resource for staff, assists in research, and works closely with management to prepare newly hired staff. Given the ever-growing needs for nursing education and development at the institution, the CNS was a welcome addition.
The 1980s
During the 1980s, clinical nursing practice kept pace with the rapid social and technical changes. Because the patient care areas within Barrow were continuing to expand, a second CNS was hired in the mid1980s. And in response to the growing nursing shortage, work schedules were modified to incorporate 12-hour shifts.
Early in the decade, intracranial pressure was monitored with a subdural Richmond bolt or a ventriculostomy. These devices were basic. The ventriculostomy was nothing more than a red rubber feeding tube connected via intravenous tubing to a separate port on a sterilized bottle that had previously been used to administer mannitol. The management of head-injured patients depended on intracranial monitors, respiratory alkalosis, administration of high-dose corticosteroids, osmotic diuretics, and induction of a pentobarbital coma. Patients who survived the initial injury were frequently transferred to the newly dedicated Head Injury Rehabilitation Unit on the third floor.
Patients with spinal cord injuries were immobilized by affixing tongs to a skeletal traction apparatus assembled at the bedside. Patients were placed on Stryker frames or Circo-electric beds that could turn side to side without disrupting spinal immobilization. Halo braces for spinal immobilization were developed in the early 1980s. By 1987, the demand for rehabilitation for spinal-cord injured patients was so great that a spinal cord injury rehabilitation unit consisting of 8 beds was opened on the fifth floor at Barrow. Furthermore, in response to the number and complexity of patients with acute spinal cord injuries, a designated neuroscience nurse educator was hired to provide nursing as well as patient and family education for this subset of patients.
Surgical obliteration was the preferred option for ruptured intracranial aneurysms. Yet the elegant techniques now associated with vascular neurosurgery had not been developed. If an aneurysm of the internal carotid artery was deemed inoperable because of its location, the patient was taken to the OR for carotid ligation or placement of a Silverstone clamp around the carotid artery in the neck. If a clamp was used, the goal was to tighten the screw daily to decrease blood flow through the carotid artery slowly. Nurses had to remain vigilant when caring for these patients, who were carefully assessed every 5 to 10 minutes for 4 hours for evidence of a frank stroke or transient ischemic attack.
Then, as now, the care of patients with a complex aneurysm was demanding. Vasospasm was still the primary concern, but the challenges were different. Nurses were often confronted with patients with vasospasm and an unclipped aneurysm. During the 1960s, 1970s, and early 1980s, surgical techniques differed dramatically from current standards. There were no microscopes, no specialized aneurysm clips, and no options for endovascular coiling. Most patients with a ruptured intracranial aneurysm developed vasospasm to various degrees, and surgical outcomes were poor if the patient underwent surgery during the period of vasospasm. Therefore, the NICU nurses were challenged to care for patients throughout the period of vasospasm with the dual goal of minimizing the risk for rebleeding while maintaining adequate cerebral perfusion. Amicar, a potent intravenous drip, was used to prevent lysis of the intracranial clot while vasospasm was treated empirically with a combination of intravenous drips: aminophylline, theophylline, Isuprel, and lidocaine. Nurses had to titrate five intravenous drips in addition to keeping the patient in a quiet, darkened room to avoid overstimulation.
In the early 1980s, patients with a ruptured intracranial basilar tip aneurysm also were nursed through the period of vasospasm. If, after 21 days, the patient was stable, arrangements were made to transport the patient via air ambulance to the Montreal Neurological Institute. Once there, their care was assumed by Dr. Charles Drake, the only neurosurgeon in North America who operated on such vascular lesions at the time. By the mid1980s, however, it was no longer necessary to transport these patients. The new Medical Director of Barrow, Dr. Robert F. Spetzler, was pioneering the art of cardiac standstill procedures for use with this patient population.
During the 1980s Barrow grew tremendously, and the renewed energy and focus on cerebrovascular disease directly affected the number of beds needed for patient care. The demand for both step-down beds and acute stroke beds also increased. Several members of the Barrow nursing staff began to work with early developers of the current EMTEK system, a computerized charting system. In addition to computers at the bedside, computers were also being used increasingly in radiology where magnetic resonance imaging (MRI) was introduced.
The 1990s-Present
In the 1990s, clinical practice was influenced by technology and by the increasing financial constraints placed on healthcare systems and providers. Within the nursing profession, the worsening nursing shortage coupled with the reduction of LPNs contributed to the demise of the Team Nursing concept and ushered in the concept of Primary Nursing. This model consisted of one RN and one aide who were assigned the complete care of four or five patients. A new method of tracking charges for patient care and procedures, diagnostic-related groups (DRGs), was accepted as the norm throughout the country and by all healthplans. DRGs mandated the amount of monies reimbursed by healthplans to participating hospitals. However, the DRGs did not account for changes in the acuity of patients, and the caseload at Barrow was typically composed of high-acuity patients. To assist with concerns such as discharge planning, the expanded role of case management was explored. Nurses with several years of experience at Barrow were hired to assist the medical care team with appropriate referral and care strategies for patients who required prolonged hospitalization.
The role of hospital-based nurse practitioners (NPs) focused on the neurosciences was developed at Barrow in the early 1990s. NPs are nurses who have completed graduate level education and are licensed to perform physical examinations; to provide patient assessment, care and management of acute and chronic illnesses; to prescribe and manage medications; to identify health needs that require referral for specialized care; and to promote health and wellness. Originally, NPs were introduced in community health clinic settings. Barrow, however, explored the option of having NPs work in the Division of Neurological Surgery to assist with the overall care of neurosurgical patients on the general wards and intermediate care area and to facilitate timely patient discharge from the hospital. No other hospitals in the country had yet employed NPs in their divisions of neurological surgery, and NPs in the field of neurosciences were unusual. Their role in the hospital setting was even less clear.
During the past decade the value of the contributions of NPs has become evident. NPs now work in an interdependent role with the nursing and surgical staff in the step-down unit, the general floor, rehabilitation, and Sav-A-Day unit. These NPs are able to perform focused and expanded patient examinations, to order appropriate diagnostic testing, to provide patient teaching, to prescribe medications, and to execute discharges in conjunction with the attending staff. This role has reduced the overall workload for the resident staff, an especially important benefit with the new mandate limiting the resident work week to 80 hours.
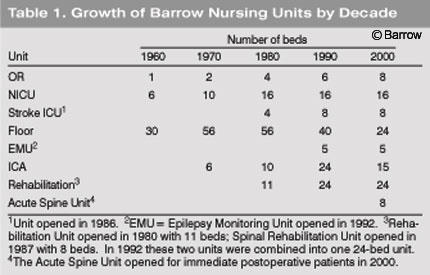
Today, Barrow has developed into a model of nursing management as evidenced by the numerous outside institutions that request formal site visits to learn from our success. All clinical areas within Barrow are united under one nursing director who is responsible for all inpatient neuroscience care areas, the emergency room, and trauma services. Such a comprehensive network of areas demands input from both management-based and clinical-based leaders to adapt to the ever-changing demands of patient care and fiscal responsibilities. The Barrow nursing staff now numbers 286 compared to the original 28 in 1962.
In addition to the expansion of nursing services, patient care units expanded (Table 1). In 1992 the Neurological Rehabilitation Unit expanded to include the Spinal Rehabilitation Unit for a total of 24 beds. The stroke ICU, initially opened in the 1980s, was firmly established in the 1990s, as was a unit for the acute care needs of postoperative spinal patients. An Epilepsy Monitoring Unit was also opened to provide continuous EEG, video, and sound recordings of patients admitted for seizure studies.
Education
Nursing Education
In 1889 Dr. Charles Mills, Chair of Neurology at Philadelphia General Hospital, recorded the earliest set of lectures on the necessary care of neuroscience patients in the United States. Dr. Joseph Collins, MD,[3] expanded Dr. Mills efforts and published an article on caring for patients with ‘nervous diseases,’ encouraging nurses to learn from books as well as from experts so they could care for patients appropriately. In 1920, Ms. G.M. Dwyer, a nurse who had previously worked with Dr. Mills, published Nursing Care Following Operations on the Spinal Cord and Brain, the first article on neuroscience nursing care published in the American Journal of Nursing.[4]
Despite these early attempts at formal instruction, no formal program of neuroscience nursing instruction evolved. In nursing schools nurses learned general nursing concepts. The central nervous system was taught in the same general format as all other major systems. Nurses therefore often graduated from school with little knowledge of or appreciation for the care of neurological patients.
In the 1960s, just as in the early part of the 20th century, nurses began to learn what they needed to know to care for patients with neurological injuries and disorders from physicians. Beginning in the early 1960s, staff neurologists and neurosurgeons at Barrow taught nurses the principles of neuroscience with informal presentations. The presentations introduced the nurses to the basics of neuroanatomy, the principles of the neurological examination, and the neurosurgical procedures performed at the time. Concepts such as increased intracranial pressure were taught by simple maneuvers such as lowering a hand and observing venous distension.
As a general rule, nurses did not learn how to be neuroscience nurses until they began working at Barrow. The exceptions were student nurses from the St. Joseph’s Hospital School of Nursing. These individuals often worked extra shifts on weekends and were assigned to the neurological units. There, working with fellow nurses, they learned the extra “something” required to become a neuroscience nurse. The early nursing students at St. Joseph’s Hospital knew what nurses today know to be true: the time and energy spent in developing camaraderie among nurses promote high standards of patient care, a sense of professional responsibility to patients and each other, and an overall commitment to the organization. Early Barrow nurses developed a healthy esprit de corps, especially when few nurses outside the neurosciences wanted to float to the area because comatose patients were perceived as depressing.
Dedicated educational programs exclusive for neuroscience nursing were rare. Programs conducted in affiliation with the Montreal Neurological Institute, the University of California at San Francisco, and the New York Neurological Institute provided 6 weeks to 6 months of dedicated neuroscience nursing lectures and limited exposure to patient care. Three nurses from Barrow were able to travel to Montreal to participate in their 6-month program. However, distance and costs precluded most nurses from being able to take advantage of this option.
Recognizing the importance of a program dedicated to developing expertise in neuroscience nursing, Barrow introduced the Neuroscience Nursing Graduate Education Course in 1985 with the support from St. Joseph’s Hospital and a generous grant from the Barrow Women’s Board. This specialized 21-week program in neuroscience nursing included a full-time course of study with classroom instruction, theory, and a corresponding clinical practicum. In addition to the initial grant that funded the program, the Women’s Board provided scholarships for Barrow nurses to attend the program. For 5 years the program was successful, attracting nurses from the hospital, the Phoenix metropolitan area, Canada, France, and Denmark. Due to space and economic constraints, the course was eventually closed.
With the introduction of the 1990s as the Decade of the Brain, emphasis on neuroscience nursing education was renewed. Due to its high regard as a clinical neuroscience center, Barrow would come to provide specialized clinical training for graduate nurses at a national level. Although the Graduate Neuroscience Nursing Program no longer exists, Barrow nurses are still actively involved in the educational process and serve as educators for nursing students or as preceptors for NP students.
Community Education
The educational efforts at Barrow extend beyond the immediate needs of nurses and inpatients. Since 1987 dedicated nurses at Barrow have been involved in community education, outreach, and injury prevention programs. Barrow has participated in the National Think First Injury Prevention Program, Stroke Prevention Coalition, Staying Alive Programs, and Feet First, First Time. Between 1995 and 2002, more than 64,000 people attended 1500 individual presentations at schools or community settings. Representation at more than 235 health fairs and exhibits has exposed an additional 119,000 people to our community health education programs. In 1987 Barrow was recognized by the Governor’s Office of Highway Safety for its Staying Alive Program. In June 2000, Barrow was recognized as a partner in the Maricopa County SAFE KIDS Program, which received an award from the Maricopa Association of Governments. Overall, Barrow has helped expose more than 184,000 individuals to educational information on the prevention of neurological disease and trauma-related dysfunction.
Professional Development
Just as the earliest roots of neuroscience nursing education were facilitated by physicians, so too was the beginning of the only professional organization for neuroscience nursing, the American Association of Neuroscience Nurses (AANN). Originally named the American Association of Neurosurgical Nurses, the organization was founded in 1961 by Agnes Marshall Walker, RN; Barbara Therrien, RN; and Dr. Paul Bucy, a member of Barrow’s founding Task Force.[8]
The first AANN meeting was held in Chicago in 1968. From across the United States, 104 nurses convened to approve the Constitution and By-Laws and to attend the presentation of two papers. No Barrow nurses presented a paper at that inaugural meeting. Since 1980, however, Barrow nurses have made five to 15 podium or poster presentations each year, thanks to the support of Barrow’s Nursing Administration and grants from the Barrow Women’s Board. Overall, Barrow nurses have made more than 100 presentations at national meetings and more than a dozen at international meetings. At the 2002 annual AANN Congress, two Barrow nurses won the award for best poster presentation (Fig. 2).
For years, Barrow nurses have been valuable and sustaining contributors to the AANN. In 1984 Barrow nurses helped establish the first local chapter of the AANN. That same chapter remains in existence as the sole chapter in Arizona, and 10 Barrow nurses have served as President of the chapter during the last 22 years. Furthermore, three Barrow nurses have represented neuroscience nursing nationally by serving as the president of the AANN (Fig. 3).
Barrow nurses have also been founding members of affiliated neuroscience nursing organizations, such as the American Board of Neuroscience Nursing (ABNN) and the Neuroscience Nursing Foundation (NNF).
The ABNN is the only national accrediting board for nurses who wish to pursue national certification as a certified neuroscience registered nurse (CNRN). After a 2-year minimum of employment in a neuroscience area and two letters of recommendation, a nurse may sit for a 4-hour examination covering all aspects of neuroscience nursing. After successfully completing the test, the nurse may use the initials of CNRN after her RN title to reflect an expert level of knowledge in the care of neuroscience patients. The CNRN certification is not life-long; it must be renewed every 5 years. In this country consumers of health care have increasingly called for board certification in specialties. The CNRN certification therefore reflects an individual’s commitment and dedication to promoting excellence in neuroscience nursing. Similar certification exists for nurses in the operating room (CNOR) and rehabilitation (CRRN). Barrow nurses have demonstrated their dedication to excellence by pursuing such certifications as evidenced by the 13 CNRNs, 3 CNORs, and 13 CRRNs on staff.
served as the President of the American Association
of Neuroscience Nurses. Left to right: Toby Anchie, RN
(1994 to 1995), Virginia Prendergast, RN (1998 to
1999), and Marilyn Ricci, RN (1984 to 1985).
Two Barrow nurses also were the founding members of the NNF, a nonprofit organization that has provided grants and scholarships to nurses studying in the neurosciences since 1995. In the past 7 years, a total of $234,000 in the form of research grants, scholarship awards, a nursing clinical research fellowship, and travel grants has been awarded to nurses nationally and internationally.
Barrow nurses are active in the World Federation of Neuroscience Nurses (WFNN), an international nursing organization organized to support and promote global excellence in neuroscience nursing. Since the inception of the WFNN in 1969, Barrow nurses have attended every WFNN meeting to present information on the care of neuroscience patients. A Barrow nurse also now serves on the Board of Directors of the WFNN and as the Treasurer of the organization.
Despite their commitment to national and international organizations, Barrow nurses recognized the need for a local symposium dedicated to neuroscience nursing. Hence, the Barrow Nursing Symposium was introduced in 1981 and has been held every year since then. Speakers are expert physicians and nurses. Throughout the decades, the focus of the symposium has been on improving the care of neuroscience patients by understanding and applying innovative techniques.
Barrow has also hosted about 20 national and international visiting nurses. On the national level, nurses with a special interest in the neurosciences who have been pursuing additional studies in the neurosciences have come to Barrow to hone their skills by working with staff nurses, CNSs, and NPs. Barrow nurses have also welcomed nurses from Europe, Canada, Australia, and Singapore in their quest to develop neuroscience nursing in their home countries.
Nursing Research
Nursing research is still under development at Barrow. Thus far, research efforts have typically been conducted as part of a nurse’s master’s thesis. Examples of such studies include changes in intracranial pressure in patients allowed to rest undisturbed compared to those who received the standard ICU care at night (Prendergast VP, unpublished data, 1985). Currently, 10 neuroscience nurses are now serving as coordinators for 55 clinical trials and other medical research projects. Altogether, Barrow nurses have been coordinators for 127 research studies. Despite their intensive clinical duties, Barrow neuroscience nurses have also found time to publish about 40 professional nursing articles.
Barrow nurses are now working toward the clinical implementation of evidence-based practice. The goal of this ongoing commitment is to base nursing practice guidelines on systematic reviews of the clinical literature. Opportunities for collaborative nursing research with Lund University in Sweden are also being explored.
Discussion
There is no substitute for the neurological assessment of patients. Different rating scales such as the Glasgow Coma Scale, National Institutes of Health Stroke Score, and the Karnofsky Scale have been developed and adopted to capture the functioning of patients at a given point in time. However, it remains incumbent on neuroscience nurses to assess changes and to detect subtle warning changes that herald a patient’s pending deterioration. The nuances of the neurological examination are the essential skills that every neuroscience nurse must acquire. However, it is not a skill that can be taught with complete reliability or accuracy. Rather, it must be honed over time and fostered by mentoring new staff.
In the early days of nursing at Barrow, the original staff nurses may have found it difficult to articulate how being a neuroscience nurse was different from being a cardiac nurse or a pulmonary nurse. In the early years, nurses working in the neurosciences were challenged with the adage “a nurse is a nurse.” A different picture emerges when nurses are asked why they remain involved in the neurosciences at Barrow for 10, 15, 20 or more years. Dedicated neuroscience nurses see themselves as individuals who do not give up: They do not lose hope. This trait does not translate to inappropriate expectations for a cure in an otherwise hopeless situation. Rather, it translates to nurses who are willing to assist patients and family members to adapt to an often dramatically different role in life. Sometimes it means translating the hope for a cure into the hope for acceptance.
Nurses may be characterized as neuroscience nurses because of their employment in a neuroscience field, because of an academic affiliation, or because they have passed the certification examination. Yet, the essence of a neuroscience nurse is less easily defined. Neuroscience nurses do not despair at the bedside. Instead, they focus energies on maintaining and restoring neurological function, helping patients and their families adapt, maximizing well-being and independence, and developing the wisdom to understand when energy should be directed toward a quiet acceptance of death when it is inevitable. A neuroscience nurse sees the possibilities and the expression of hope rather than a patient who appears to be incapable of doing anything. Patients need well-educated nurses who are certified in their area of expertise, who possess the underpinings of neuroscience nursing care, who are committed to excellence, and who have a passion for their work, whether at the bedside or working as NPs, educators, or researchers.
Future advances in technology will be used to expand web-based neuroscience nursing, to develop Barrow Neuroscience Nursing Standards of Care based on evidenced-based models, and to continue to promote and support excellence in nursing care. While the scope of neuroscience nursing expands at Barrow, the challenge of providing expert nursing care will remain. Advances in surgical techniques, pharmacology, or imaging techniques help improve patient care, but there is no substitute for the element of human touch, compassion, and care that nurses offer. The legacy of the Barrow nurses who began neuroscience nursing in the 1960s has been and will continue to be expressed as an ongoing dedication to patient care.
Acknowledgments
The author thanks Hal Pittman, MD, for providing historical photographs and Toby Anchie, RN; Carol Blazier, RN; Carol Browner, RN; Bonnie Duncan, RN; Marilyn Hutcherson, RN; Mary Jo Jerde, RN; Marie King, RN; Thekla Long, RN; Shirley Ofstedahl, RN; Lucy Ranus, RN; Marilyn Ricci, RN; Monica Sargent, RN; and Julie Ward, RN, for graciously answering questions and providing historical information.
References
- Anonymous: NICUs make their debut. RN 38:8, 1975
- Cammermeyer M: Serving in Silence. New York: Viking/Penguin, 1994
- Collins J: Nursing in nervous diseases: The teaching in neurological hospital. AJN 11:434, 1911
- Dwyer GM: Nursing care following operations on spinal cord and brain. AN 20:613, 1920
- Haggard HW: The Doctor in History. New Haven, CT: Yale University Press, 1934
- Hartshorn JC: Aspects of the historical development of neuroscience nursing. J Neurosci Nurs 18:45-48, 1986
- Harvey AM: Neurosurgical genius – Walter Edward Dandy. Johns Hopkins Med J 135:358-368, 1974
- Marshall AM: The birth of an association. J Neurosurg Nurs 10:146-149, 1978